The asterisk (*) denotes his corresponding authorship.
The idealism of a hemodynamic software
The complexity of hemodynamic models has prevented clinicians from getting the insights out of the models when relating the clinical issues with the hemodynamic model. Visualization is the most persuasive way to illustrate a hemodynamic equation, and simulation is needed to visualize how the equation changes upon the manipulation of the coefficient of equations. Thus, the success of the hemodynamic software depends on how easy it is to work with visualizing the hemodynamic model and how effective it is for clinicians to draw insights from the models.
Additionally, it would be better if the following conditions are fulfilled: -1) an engineer takes care of the CPU time and memory management when combining and implementing numerous hemodynamic models published so far; -2) the simulation software provides an alternative interface other than GUI, which could enable experts to work more flexibly with the hemodynamic model; -3) components such as device interface, medical statistics, and artificial intelligence are coherently integrated in order to facilitate hemodynamic research.
Infrastructural aspects of each component
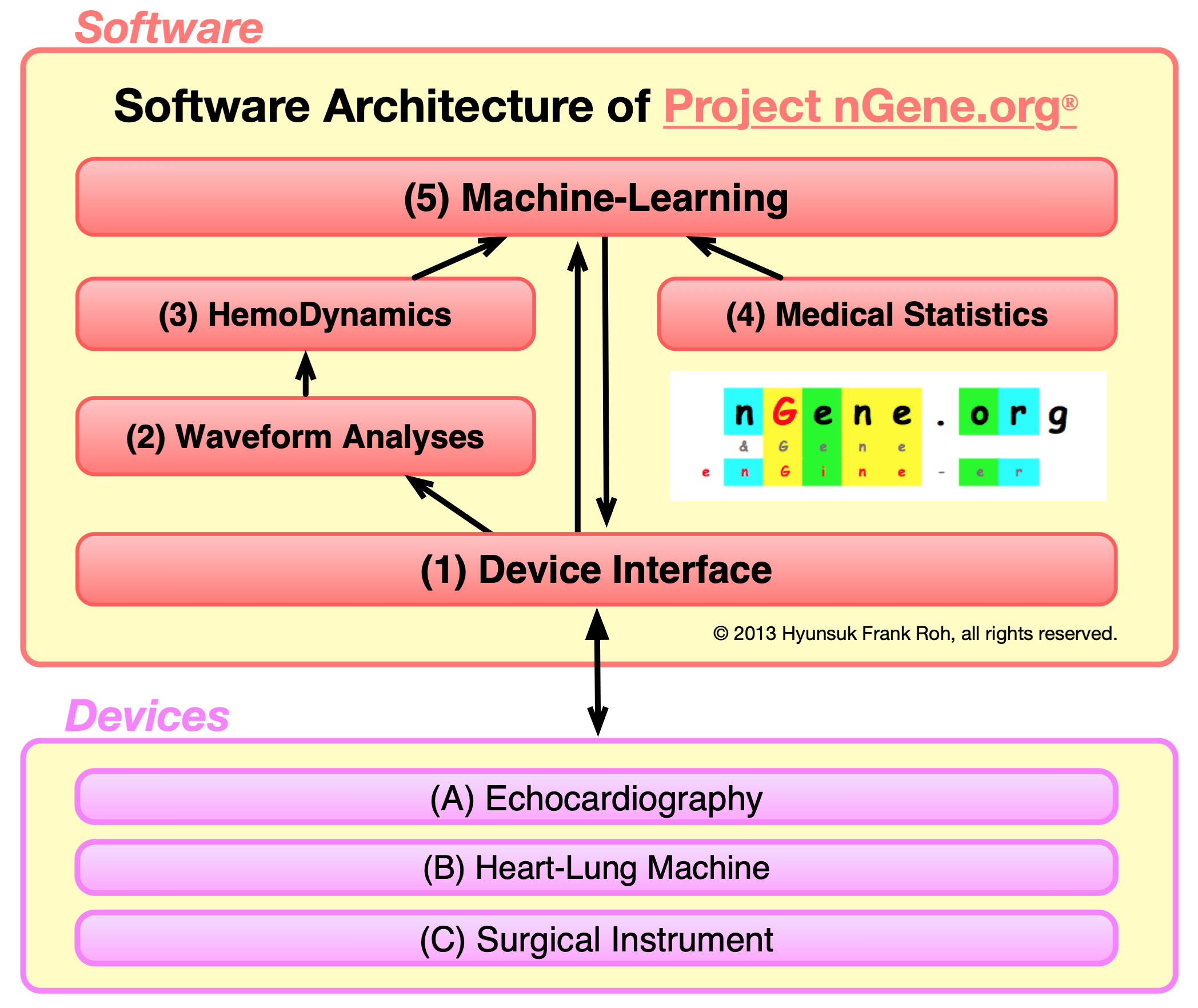
Each component will be the basis upon which other components can be built. This circulative data flow in the architecture diagram will eventually contribute to the development of other components synergistically. In other words, when considering the final overall goal of this software project as facilitating the data flow according to the software architecture, one part of the development will benefit the other part of the research.
The hemodynamic workbench software will be implemented to provide the following infrastructural functionalities: (1) To receive signals from the hemodynamic instrument; (2) To extract necessary information by wavelet analyses; (3) To understand the data according to the hemodynamic model and simulation; (4) To provide medical statistics; (5) To perform an action by reinforcement of the learning process.
Why the thoracic cavity for hemodynamic software and robotic surgery?
The thoracic cavity is intriguing in regards to its demanding physiological and computational potential. It is physiologically intriguing how the lungs and the heart are directly governed by the laws of physics: the hemodynamics during blood circulation and respiration with relation to auscultation, electrocardiography, ECMO and anesthetic machines. Computationally, a kernel-level device driver and Bayesian-based machine learning algorithm can be employed for (1) monitoring of the states of the thoracic organs, (2) computer-assisted hemodynamic modeling and simulation, and (3) machine learning for information processing. In addition, the thoracic cavity is ideal for a specialty that sits on the cusp between surgery and engineering to perform intellectually and technically challenging surgical robotic R&D projects on the organs encased by bones, which are best accessed and manipulated by a thin robotic hand instrument with ergonomic advantages. This will widen the indication of robotic cardiovascular surgery with new surgical procedures that integrate various additional hemodynamic devices and computational support.
"Surgeons must progress beyond the traditional techniques of cutting and sewing that have been their province since surgeons were barbers to a future in which approaches involving minimal access to the abdominal cavity are only the beginning." - Pappas et al. (2004) N Engl J Med.
Device driver interface component will enable the software to access raw data directly from a device. Biomedical companies seem to welcome the idea of enabling third parties to write software for their devices, which is exemplified by 3M providing an SDK (Software Development Kit) to allow people to write software for its Bluetooth stethoscope. However, my ultimate goal will be to make one step further by implementing the kernel-level device driver that would connect devices more fundamentally (as compared to existing SDK) and, therefore, to establish an integrative and flexible hemodynamic workbench.
Some EKG classification articles (Lee, 2013) (Lihuang, 2010) relied exclusively on the MIT-BIH arrhythmia database or the standard test material to evaluate their arrhythmia detection algorithms. However, to the best of our knowledge, the difficulty of acquiring additional new raw EKG dataset due to the absence of open-source device interface for EKG instrument may be at least partially attributed to those researchers's having to work exclusively on MIT-BIH arrhythmia database. Therefore, if this software can receive the EKG raw stream over a WiFi or USB connection from instruments, future engineers can acquire additional test materials by collecting further raw EKG data alongside with corresponding EKG diagnoses, directly.
Nonetheless, companies would be cautious about opening their device protocols for my implementing the kernel-level device interface, since doing so might change the company's marketing strategies and policies. Therefore, continuous improvement of Project nGene.org® in the long-term to gain agreement concerning its clinical pragmatism and to embrace clinicians' needs by providing an easy-to-write environment for their own scripts will have to be prioritized over this kernel component.
"(2) Waveform Analyses" component pre-processes the raw wavelet data directly from the devices via the "(1) Device interface" component. In order to handle the raw wavelet dataset, such as EKG, lung and heart sounds, etc., two core algorithms have been chosen to be common denominating features: Independent Component Analysis (ICA) separates the mixed wavelets, whereas Support Vector Machine (SVM) classifies things after being trained.
Its benefit can be illustrated by how this feature may change the existing flow. These machine-learning components can be used tentatively, until a more precise implementation of the classification for wavelets is implemented later in the point of time. For example, machine-learning algorithms for classifying EKG would be no match for a manually-written conditional statements implemented according to the Sokolow-Lyon Criteria for left ventricular hypertrophy (LVH) (Sokolow, 1949), as it would be nonsensical for training SVM to distinguish whether the summation of the S wave in V1 and the R wave in V5 or V6 is greater than, specifically, 35mm or not for LVH. However, until the manually-implemented code is developed according to certain criteria, it may be better to employ machine-learning features to accommodate wavelets in order to accelerate research and development in the meanwhile.
For an example of embedding this software into the educational CPR kit mentioned above, the AED (Automated External Defibrillation) algorithm requires distinguishing normal EKG from various arrhythmia cases. However, since the MIT-BIH "arrhythmia" database does not have normal EKG dataset, the "(1) Device Interface" component can be used to collect a normal EKG raw dataset. Once normal EKG data with diagnoses are accumulated, then the SVM algorithm can be trained to classify whether it should be defibrillated, synchronized cardioversion, non-shockable, and normal, until the development of a more accurate manually-programmed classifying algorithm.
Project nGene.org® intends to facilitate research on the hemodynamic model, not only to better understand the physiology, and but also to gain further insights into improving the model. There are numerous equations published already and in the future and it may be too late if we just wait for the echocardiography manufacturing engineer to implement the module for the equation we need. Unless it is open-sourced, it cannot possibly follow the speed of insights during research. Yale Neuron is open-sourced with GUI for simulating neuron network; however, in my opinion, no matter how flexibly a software architect may implement its GUI, it cannot be on a par with the flexibility and creativity of new equations and insights of clinicians in the future.
Therefore, Project nGene.org® tries to circumvent this problem by integrating R script so that clinicians can add their equations to test those features during echocardiographic measurements on the flies. At the same time, I believe that the success of earning popularity depends on how easy and generic it is for clinicians to add and modify the source code. Since clinicians do not have time to spend on learning, it is very important to make it very intuitive to make them willing to invest their time. I think that clinicians will invest their time only if they can get it intuitively.
(4) Medical Statistics & (5) Machine Learningindex
"(4) Medical Statistics" is something that I do, not as a destination, but as a necessary step. To put it straightforwardly, the ultimate goal is "(5) Machine Learning". "(5) Machine Learning" component is pushed back on the priority list in the Masterplan Chart, because the software is designed to provide the following different types of dataset for the machine-learning algorithms: (i) Directly from hardware via the kernel program part, "(1) Device Interface"; (ii) Indirectly processing the wavelets raw data from instruments, "(2) Waveform Analyses"; (iii) Parsing and processing articles, especially meta-analysis and survival curve data, "(4) Medical Statistics", via a semantic web.
The semantic web is a very suitable piece for medicine due to several reasons: (1) It is very flexible to integrate other semantic webs together, such that it can be used as a knowledge database with numerical information. (2) This numerical information with a network form can be fed into Bayesian-based machine learning. (3) Meta-Analysis is one of the forms of very specialized information that are available in the domain of medicine, and getting the hazard ratio from the survival curve for meta-analysis was, in my opinion, the most difficult methodology and the most challenging technical barrier when building a semantic web database.
Software Architecture (The 2024 Edition)
As both a medical doctor and a software engineer, with experience in echocardiography and serving as an IRB chair, I bring a unique, chimeric perspective to the development of Project nGene.org®. This dual expertise is crucial in navigating the challenges outlined in three seminal works: The Mythical Man-Month, The Innovator's Prescription, and Crossing the Chasm.
The Mythical Man-Month: In the interdisciplinary world of software and medicine, I have learned that communication is key to bridging the gap between different fields—what I call the "Apple and Orange" problem. This lesson was driven home by my experiences and reinforced by Fred Brooks' The Mythical Man-Month. Brooks warns that simply adding more manpower to a project often increases complexity rather than reducing it. As a chimera, trained in both fields, I strive to minimize this intercommunication complexity, ensuring that the app remains manageable and effective without the need to constantly increase resources.
The Innovator's Prescription: The Project nGene.org app is not designed to guarantee perfect accuracy in recognizing visual or auditory data through its camera or microphone. Instead, drawing from The Innovator's Prescription, the app's primary objective is to disrupt traditional clinical workflows by simplifying and democratizing complex medical processes. My goal is to enhance the clinical experience, making it more efficient and cost-effective, while keeping the app accessible to a broader audience. Additionally, by making parts of the codebase open-source, we are fostering a collaborative environment that invites continuous innovation and improvement.
Crossing the Chasm: Finally, in alignment with Geoffrey Moore's Crossing the Chasm, this app is strategically focused on identifying and capturing its niche market within the healthcare industry. By targeting a specific segment that values innovation, efficiency, and cost-effectiveness, the app aims to establish a strong foothold and gradually expand its user base. I am committed to ensuring that the app not only provides core technology but also offers a comprehensive ecosystem of support and services. This approach ensures seamless integration into existing clinical workflows, addressing the pragmatic needs of a broader user group and facilitating the app's transition from early adopters to the early majority.
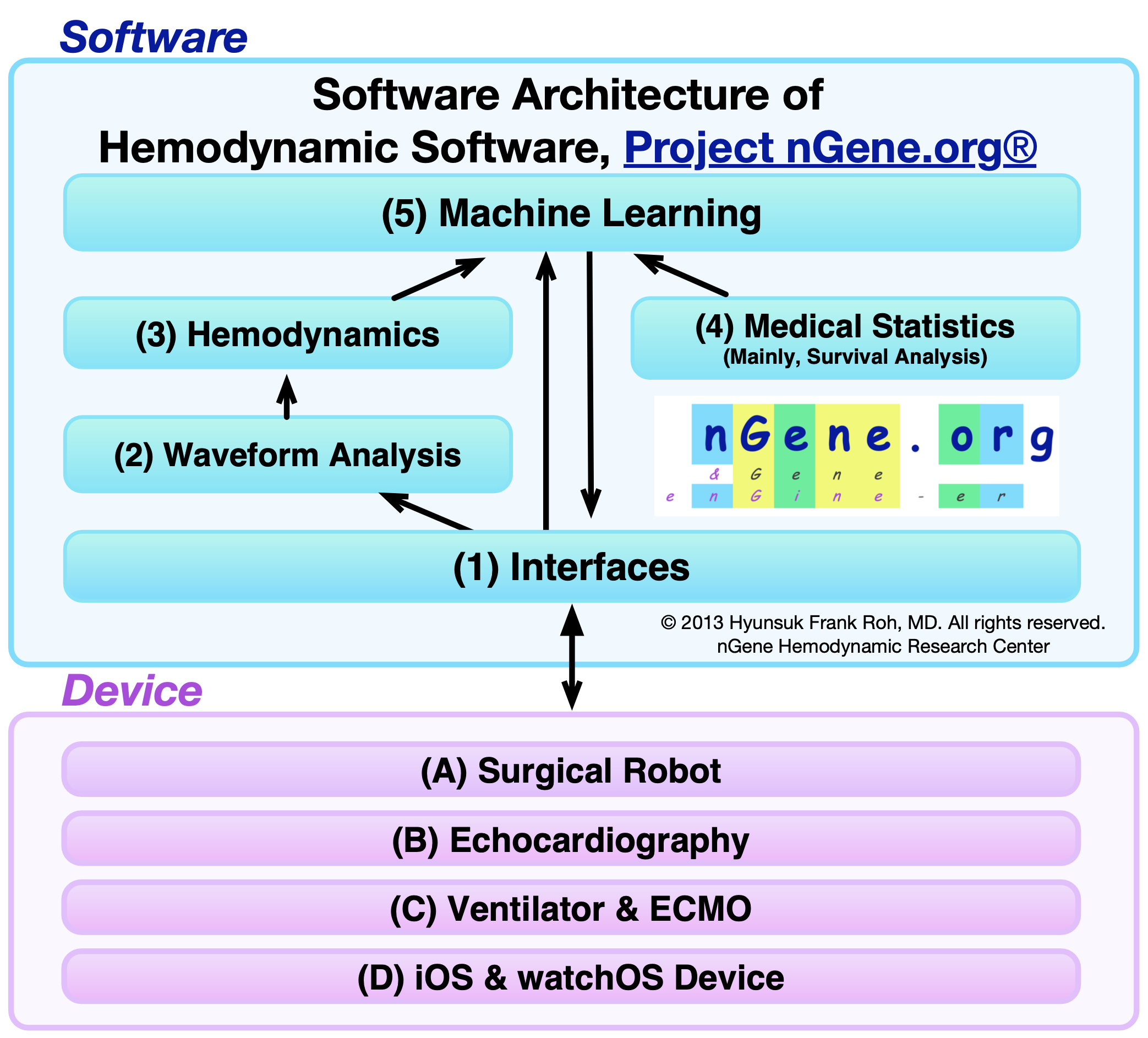
The software project is meticulously crafted, with each component acting as a foundational pillar for subsequent innovations, establishing a circular data flow within its architectural framework. This methodology is anticipated to synergistically propel the evolution of the platform's elements. The project's paramount objective is to refine data circulation to mirror its architectural blueprint, ensuring that progress in one domain reciprocally amplifies research endeavors across the board. The hemodynamic workbench software is poised to offer essential functionalities: (1) capturing signals from hemodynamic instruments, (2) distilling vital information via wavelet analyses, (3) decoding data through hemodynamic models and simulations, (4) compiling medical statistics, and (5) executing actions based on a reinforcement learning algorithm.
Implementing the software marks the recrystallization of his professional journey, serving as a compass to navigate his career. This endeavor will not only guide him towards new horizons but also enrich his understanding for further development, ultimately fulfilling his life's purpose and enhancing his sense of satisfaction.
Why the thoracic cavity for hemodynamic software and robotic surgery?
The thoracic cavity, encasing critical organs such as the heart and lungs, presents a unique intersection of physiology and technology, demonstrating the profound influence of physical laws on biological functions. From a computational perspective, the integration of kernel-level device drivers with machine learning algorithms offers transformative potential in thoracic medicine. These technologies enable continuous monitoring of thoracic organ states through advanced waveform analyses, including ECG and ventilation monitoring waveforms (pressure, flow, volume), and auscultated mixed heart and lung sounds. Such detailed data acquisition is crucial for effective decision-making and patient management in real-time scenarios. The computational modeling capabilities, particularly in hemodynamic simulations, are further enhanced by incorporating echocardiography data. This integration is especially pivotal in addressing complex conditions like pulmonary hypertension, where accurate hemodynamic models can significantly improve the outcomes of interventions such as congenital heart defect surgeries in neonates. By simulating various physiological conditions, surgeons and clinicians can predict the effects of surgical interventions, thereby planning surgeries with higher precision and better prognostic outcomes. Moreover, the field of robotic surgery in the thoracic cavity is advancing rapidly, driven by machine learning algorithms that learn from thousands of surgeries performed by human doctors. This data not only informs the development of autonomous surgical robots but also supports the creation of new surgical techniques that integrate hemodynamic devices and computational support. The advent of slender robotic hand instruments designed specifically for the ergonomic constraints of thoracic surgery further underscores the technical sophistication in this field.
"Surgeons must progress beyond the traditional techniques of cutting and sewing that have been their province since surgeons were barbers to a future in which approaches involving minimal access to the abdominal cavity are only the beginning." - Pappas et al. (2004) N Engl J Med.
The integration of computational modeling and simulation has revolutionized the field of hemodynamics, transforming the way cardiovascular conditions are studied and treated. The dynamic and interactive nature of hemodynamic simulations, as discussed in "Computational Thinking" by Peter J. Denning and Matti Tedre, goes beyond the capabilities of traditional graph drawing, which often falls short when dealing with the complex, variable nature of biological systems. Unlike static graphs that display a fixed dataset, simulations provide a real-time, interactive platform that allows researchers to modify parameters and observe how these changes affect the cardiovascular system. This interactivity is crucial for a detailed understanding of how blood flow and pressure react to various physiological changes, making simulations an indispensable tool in predicting the effects of alterations within the cardiovascular system and aiding in the development of effective treatments for heart diseases.
Advanced modeling and simulation techniques are particularly impactful in addressing the challenges of congenital heart defects (CHD) and pulmonary arterial hypertension (PAH). For instance, the development of logistic-based equations for estimating Pulmonary Artery Pressure (PAP), as noted in Project nGene.org®, underscores the practical application of theoretical models in a clinical setting. These simulations enable the visualization and analysis of cardiovascular responses to treatments in a risk-free environment, which is especially crucial in designing interventions for vulnerable populations such as neonates with CHD. The traditional approach to surgical interventions, fraught with significant risks, highlights the need for non-invasive methods facilitated by simulations. By simulating specific cardiovascular conditions associated with CHD and PAH, Project nGene.org® not only provides insights into the intricate factors influencing patient outcomes but also enhances the potential for successful treatments while minimizing risks.
The ongoing initiative to harness hemodynamic modeling and simulation in the development of neonatal CHD surgery simulations exemplifies the shift towards simulation-based planning and execution of surgical interventions. This approach not only refines the understanding and management of PAH within the context of CHD but also pioneers new methodologies for surgical planning. By creating highly accurate, virtual models where surgical strategies can be tested and refined, simulations ensure the highest level of safety and efficacy in neonatal CHD treatments.
(4) Medical Statistics & (5) Machine Learningindex
Integrating "(4) Medical Statistics" into my work is not merely a destination but a vital step towards a broader objective: mastering "(5) Machine Learning". This component is strategically deferred in the Masterplan Chart, as the software is intricately designed to curate diverse datasets for machine learning algorithms through various means: (i) directly from hardware via the kernel in the "(1) Device Interface"; (ii) by processing raw wavelet data from instruments in "(2) Waveform Analyses"; and (iii) by parsing and analyzing medical literature, particularly meta-analyses and survival curve data, through "(4) Medical Statistics", utilizing a semantic web (or Web 3.0) approach. Initially, the semantic web seemed perfectly aligned with medical applications for several reasons: (1) Its inherent flexibility facilitates the integration of multiple semantic webs, creating a comprehensive knowledge database enriched with numerical data. (2) This numerically dense network is ideal for Bayesian-based machine learning applications. (3) Specifically, meta-analysis represents a form of highly specialized information within the medical domain, where deriving hazard ratios from survival curves posed a significant technical challenge and a methodological bottleneck in developing a semantic web database.
However, the rapid evolution of machine learning algorithms necessitated a shift in methodological approach. Acknowledging the advancements in deep neural networks and linear algebra techniques, especially Singular Value Decomposition (SVD), these methods now appear more apt for these objectives. This change in methodology is driven by the emerging efficiencies and capabilities of these algorithms in machine learning, signifying a pivotal adaptation to the evolving landscape of data analysis. This recalibration of approach, moving from a Bayesian-based semantic web to emphasizing deep learning and SVD, reflects a commitment to leveraging the most effective and advanced methodologies available in the field of machine learning. It underlines readiness to adapt and evolve in response to the dynamic nature of technological advancement and the continuous quest for more refined and powerful analytical tools.
The reconsideration of Bayesian algorithms also draws from a historical challenge in the field of artificial intelligence. Despite the Bayesian approach's flexibility and appeal, its application is marred by complexity in calculations beyond simple, restrictive assumptions. This complexity often necessitates approximation methods or sampling, which, while practical, diverge from dealing with the real posterior distribution directly. Further complicating the landscape was the neural network's initial inability to solve the exclusive OR (XOR) problem, a straightforward task achievable with basic digital logic gates but unattainable by a single-layer perceptron. Although it was known that multi-layer perceptrons could theoretically execute such tasks, the lack of effective training methods led to significant disillusionment and a temporary retreat from neural network research. This historical bottleneck highlights the limitations of early machine learning approaches and underlines the strategic pivot towards more advanced and capable methodologies, such as deep learning, that have since overcome these early challenges. (On February 5th, 2024, this segment of the software architecture underwent a revision to include sophisticated deep learning and SVD techniques.)
Robotic Surgery
RCT Meta-analysis: Robotic vs. Laparoscopic Surgery (Frank, 2018)
Importance This review provides a comprehensive comparison of treatment outcomes between robot- assisted laparoscopic surgery (RLS) and conventional laparoscopic surgery (CLS) based on randomly-controlled trials (RCTs).
Objectives We employed RCTs to provide a systematic review that will enable the relevant community to weigh the effectiveness and efficacy of surgical robotics in controversial fields on surgical procedures both overall and on each individual surgical procedure.
Evidence review A search was conducted for RCTs in PubMed, EMBASE, and Cochrane databases from 1981 to 2016. Among a total of 1,517 articles, 27 clinical reports with a mean sample size of 65 patients per report (32.7 patients who underwent RLS and 32.5 who underwent CLS), met the inclusion criteria.
Findings RLS shows significant advantages in total operative time, net operative time, total complica- tion rate, and operative cost (p < 0.05 in all cases), whereas the estimated blood loss was less in RLS (p < 0.05). As subgroup analyses, conversion rate on colectomy and length of hospital stay on hysterectomy statistically favors RLS (p < 0.05).
Conclusions Despite higher operative cost, RLS does not result in statistically better treatment outcomes, with the exception of lower estimated blood loss. Operative time and total complication rate are significantly more favorable with CLS.
Robotic surgery cost, under the hood
Regarding the cost-effectiveness of robot-assisted laparoscopic surgery (RLS), it is generally perceived as more expensive. This perception raises questions about the viability of further employing RLS, especially amid concerns over its advantages in complications, conversion rates, and the extended operative time. However, from a patient's perspective, although numerous articles have closely compared the total operative costs between RLS and conventional laparoscopic surgery (CLS), finding a common objective ground is complicated—not to mention considering the exchange rate at the time of surgery (Morino, 2006). Moreover, the information may not be practically relevant to patients, as the total operation cost does not directly correlate with the actual payment by patients due to varying insurance policies across different companies, hospitals, and countries. Aboumarzouk et al. highlighted in their meta-analysis that the so-called 'total cost' fails to account for the 'social cost analysis', which considers the benefits of quicker recovery and shorter convalescence (Aboumarzouk, 2012).
Similarly, from the hospitals' perspective, the profitability of RLS should take into account not only the quantitative aspects such as the cost of equipment, operation time, training surgeons for both CLS and RLS considering their respective learning curves, and the impact of RLS's longer operative time on hospital revenue, hospital stay, blood loss, and insurance policies, but also qualitative factors. These include the surgeon's safety from infections like HIV, repeated radioactive exposure from bedside X-rays, and the comfort of surgeons during surgery by allowing them to sit. Lin et al. also noted that insufficient data and significant heterogeneity due to differences in skill, the extent of lymph node dissection, and the duration of the learning curve preclude a comprehensive meta-analysis of cost-effectiveness (Lin, 2011). Moreover, the unique capability of RLS for remote surgery in scenarios like war and rural areas should not be overlooked. Furthermore, it is empirically understood that the cost of new technology tends to decrease over decades. From the perspective of the public or investors in surgical robotics, it is advisable to consider these underlying factors when evaluating the cost-effectiveness of robotic surgery.
My general subjective opinion on surgical robotics
It may be surprising that the criticisms leveled at laparoscopic pioneers between the 1950s and 1990s bear a striking resemblance to those currently directed at surgical robotics. Most of the criticisms of conventional laparoscopic surgery (CLS), including 'higher complication rates than laparotomies ... attributable mainly to inexperience, and [e]ach procedure normally done via laparotomy [being] re-invented [with] trial and error,' (Page, 2008) are similarly applicable to robot-assisted laparoscopic surgery (RLS). Despite the harsh criticisms in the late 20th century, CLS has now become widely acknowledged as an indispensable surgical method (Pappas, 2004). Thus, mirroring the history of CLS, there remains the potential for RLS to achieve better clinical outcomes in the future, as knowledge and experience continue to accumulate through trial and error across society. This is especially relevant considering that the industry has now entered the era of Industry 4.0, or robotics.
ECMO (ExtraCorporeal Membrane Oxygenation)
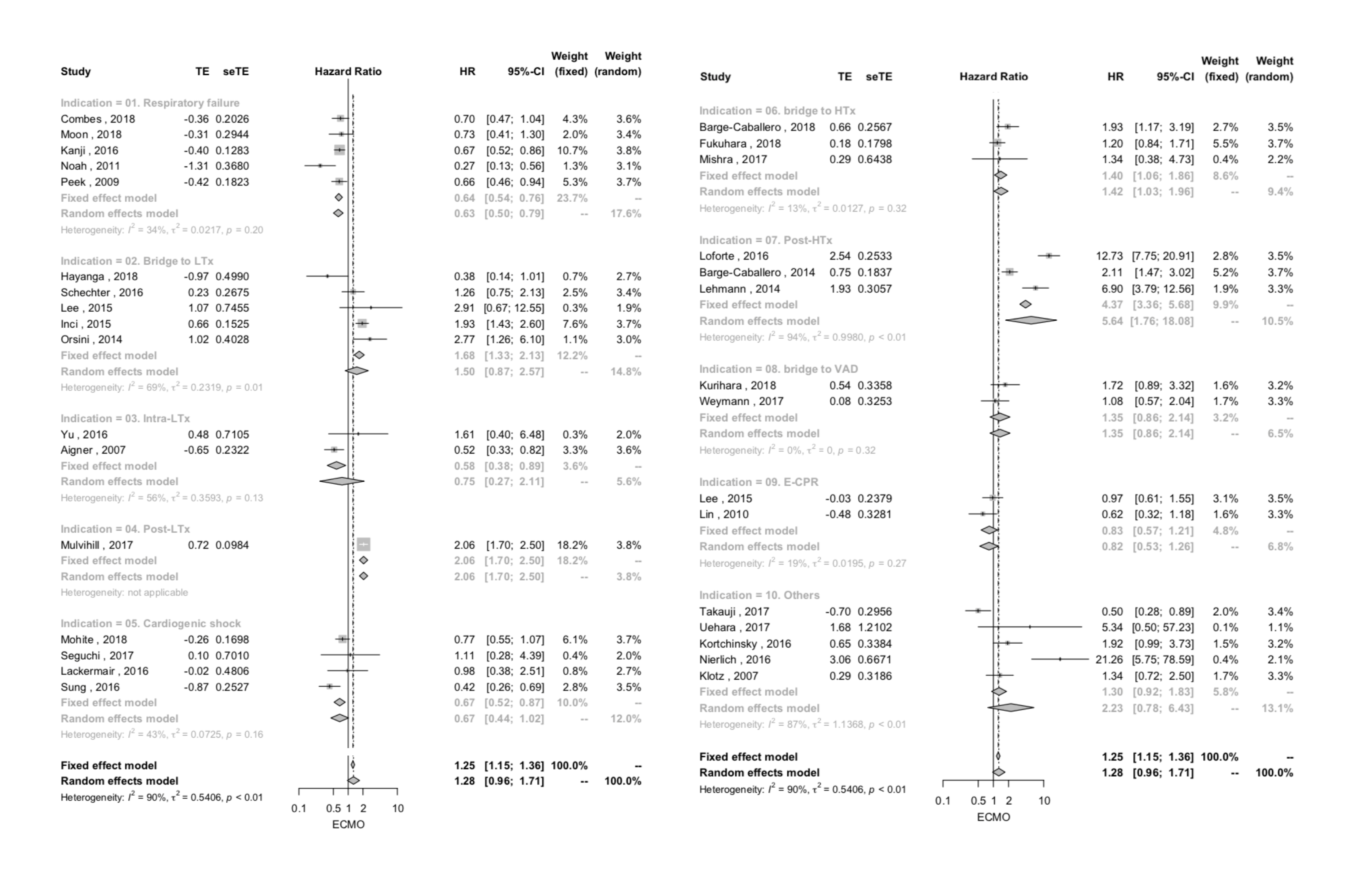
ECMO meta-analysis on hazard ratios: Cardiopulmonary Diseases (Frank, 2020)
Extracorporeal membrane oxygenation meta-analysis of time-to-event data in cardiopulmonary disease in adults
In recognition of the benefits of extracorporeal membrane oxygenation (ECMO)[1], clinical outcomes have been the subject of multiple meta-analyses. Previous meta-analyses of ECMO treatment reported forest plots based on relative risks. Unlike a hazard ratio (HR), a relative risk does not consider the time to event and censoring and runs the risk of not using all the available information[2]. In other words, with respect to the patient mortality, the relative risk between ECMO and no-ECMO patient groups cannot avoid overlooking the critical factor of how ECMO has influenced the timing of each event or patient death over the course of disease progression.
Previous meta-analyses have focused on a single indication presumably because, given the wide range of potential applications for ECMO, studying a particular patient population separately is a crucial step in terms of reducing confounding factors. The present study endeavors to investigate ECMO indications of cardiopulmonary disease as a whole and to list the findings of ECMO mortality in individual indications as subgroup analyses. This was done to ensure that a positive result of a particular indication is not automatically applied to a different patient population that may not have the same benefit, and thereby to prevent a potentially unnecessary intervention. Based on the ECMO indications[3, 4], the present study applies time-to-event data to evaluations of both the overall and individual cardiopulmonary indications of ECMO in adult patients in relation to relevant meta-analyses.
To the best of our knowledge, the present meta-analysis is the first attempt to use time-to-event HR data to illustrate a forest plot of all-cause mortality from the use of ECMO in adult patients, in terms of both overall cardiopulmonary indications and individual indications as a subgroup analysis. As shown by the results of the overall analysis, across various indications of ECMO in cardiopulmonary diseases in adults, outcomes favored neither the ECMO group nor the no-ECMO group. However, as to the subgroup analyses, the reduction in mortality in the ECMO group was found in respiratory failure, whereas increased mortality in the ECMO group was noted in post-LTx, bridge to HTx, and post-HTx.
These results should be understood not only in the context of weighing the benefits and adverse effects of ECMO, but also in consideration of patient selection issues. We could not help but notice the propensity to allocate the ECMO treatment to the poor patient conditions. In other words, the no-ECMO groups were selected and specified as groups of patients who required no invasive support[23, 24, 49]. Presumably, this was so because, in a daily practice, ECMO are used in desperate cases such as a cardiogenic shock where, without ECMO implantation, the mortality is critically high. This discriminate propensity of ECMO allocation appears to reflect the wide recognition of the benefits of ECMO treatments[1]but, at the same time, indicates a patient selection bias issue of a meta-analysis on the retrospective studies. Therefore, in addition to the intrinsic benefits and adverse effects of ECMO treatment, biased allocation of ECMO based on patient conditions as a whole appeared to contribute to the aforementioned results.
In this regard, the significant reduction in mortality of the ECMO group in the patients with respiratory failure compared with the no-ECMO group is worthy of mention. That is, against the patient selection biases that presumably favor the superior outcome in the no-ECMO group, the significantly improved patient outcomes in respiratory failure in the concurring ECMO group is evident. Our result favoring the ECMO group in respiratory failure is consistent with previous meta-analyses for H1N1 pneumonia[65]and ARDS[66]. It can be tentatively proposed thatthe inclusion of the two RCTs, which is less apt to be influenced by the patient selection bias, may contribute to the significant reduction in mortalityof the forest plot due to the increased statistical power of the pooled studies. In addition,Annichet al.stated that themajority of patients with respiratory failure including ARDS has been well supported with veno-venous (V-V) ECMO[1]. In this regard, the increased likelihood of normal cardiac function in respiratory failure conditions could enable the more frequent use of V-V ECMO (or all the use of V-V ECMO[22]), which could avoid the complications of veno-arterial (V-A) ECMO, such as systemic embolization, arterial trauma, and increased left ventricular afterload[67, 68]. However, in consideration ofnumerous possible confounding factors of heterogeneities that may have influenced the mortality results, this hypothesisneeds to be enlightened by more meticulous reasoning that unleashes which factorscontributed to this deviation of respiratory failure subgroup analysis from the overall global analysis.
Although we are aware of the fact that other ECMO meta-analyses conducted database searches on PubMed, EMBASE, Cochrane, and so forth, we searched against the PubMed database only[69], due to the following reasons. During the pilot study, we found that this study required quite an inclusive search of keywords for various cardiopulmonary ECMO indications, compared with meta-analyses on a single indication, as manifested by the total number of articles we worked with. In addition, unlike meta-analyses on relative risks and mean differences, a full-text was laboriously required to confidently make a decision to exclude its corresponding article, because the survival analysis is usually not the main topic of the referenced study but typically comprising just one line of hazard ratio information in the result table or one Kaplan-Meier survival curve figure. Nonetheless, we acknowledge that the risk of missing appropriate articles by not searching against multiple databases could have lowered the reliability of our study[70].
Whenever HRs and their variances were not reported explicitly, we estimated them from the information reported in the studies. Therefore, the significance of the results of the forest plot should have been diminished by our estimates of HR and variances. In further research, reporting numerical hazard ratios explicitly to facilitate later meta-analysis should be encouraged to investigate the mortality associated with ECMO use.
ECMO meta-analysis on hazard ratios: Respiratory failure (Frank, 2020)
Extracorporeal membrane oxygenation meta-analysis of time-to-event data in respiratory failure in adults
In recognition of the benefits of extracorporeal membrane oxygenation (ECMO) [1], clinical outcomes have been the subject of multiple meta-analyses. Respiratory failure incorporates 'oxygenation failure' of acquiring oxygen and 'ventilatory failure' of eliminating carbon dioxide [2], which are, respectively, exemplified to ECMO indications of "acute respiratory disease syndrome" (ARDS) and "hypercapnic respiratory failure" [3, 4]. The controversial efficacy of ECMO on patient mortality in respiratory failure has been statistically assessed by previous meta-analyses based on relative risks [5-9].
Unlike a hazard ratio (HR), the relative risk does not consider the time to event or censoring and runs the risk of not using all the available information [10]. In other words, with respect to patient mortality, the relative risk between ECMO and non-ECMO patient groups cannot avoid overlooking the critical factor of how ECMO has influenced the timing of each event or patient death over the course of disease progression. In consideration of heterogeneities such as veno-arterial (VA) and veno-venous (VV) types, this present study applies time-to-event data to evaluations of the utility of ECMO in patients with respiratory failure.
To the best of our knowledge, the present meta-analysis is the first attempt to use time-to-event data to illustrate a forest plot of mortality from the use of ECMO in adult patients, comprising both VA type and a majority of VV type, in respiratory failure of 'oxygenation failure' and 'ventilatory failure', compared against no ECMO group. When confining to only VV-ECMO, significant reduction in mortality was also noted.
These results should be understood not only in the context of weighing the benefits and adverse effects of ECMO, but also in consideration of patient selection issues. Although the propensity to allocate the ECMO treatment to poor patient condition was not explicitly located in the referenced studies [27-31], the non-ECMO groups were reportedly selected and specified as groups of patients who required no invasive support [33-35]. This discriminate propensity of ECMO allocation appears to reflect the wide recognition of the benefits of ECMO treatments [1] but, at the same time, indicates a patient selection bias issue of a meta-analysis on the retrospective studies. Therefore, in addition to the intrinsic benefits and adverse effects of ECMO treatment, biased allocation of ECMO based on patient conditions as a whole appeared to contribute to the aforementioned results.
In this regard, the significant reduction in mortality of the ECMO group in the patients with respiratory failure compared with the non-ECMO group is worthy of mention. Although VV-ECMO could avoid the complications of VA-ECMO, such as systemic embolization, arterial trauma, and increased left ventricular afterload [36, 37], even VV-ECMO alone is still associated with risk of haemorrhage [27, 28, 30] and circuit-associated complications [5]. That is, against the known complications of the ECMOs and the patient selection biases that presumably favor the superior outcome in the non-ECMO group, the significantly improved patient outcomes in respiratory failure in the ECMO group is evident. Our result favoring the ECMO group in respiratory failure is consistent with previous meta-analyses for H1N1 pneumonia [7] and ARDS [5]. It can be tentatively proposed that the inclusion of the two RCTs, which is less apt to be influenced by the patient selection bias, may partially contribute to the significant reduction in mortality of the forest plot due to the increased statistical power of the pooled studies. In addition, the majority of ECMO in the referenced studies was veno-venous type, possibly due to the increased likelihood of normal cardiac function in respiratory failure conditions, which enable the more frequent use of VV-ECMO (or only the use of VV-ECMO [30]) and could avoid the complications of VA-ECMO. However, in consideration of numerous possible confounding factors of heterogeneities that may have influenced the mortality results, this hypothesis needs to be enlightened by more meticulous reasoning which unleashes what factors contributed to the positive results of respiratory failure indication.
In reality, the number of ECMO studies tend to be small compared to those on relative risks, and relevant mortality studies on ECMO were not always explicitly designed to meet one subcategory of respiratory failure classification, such as 'ARDS' and 'acute respiratory failure', strictly and mutually exclusively. Thus, the scope of this current study on respiratory failure comprises mortality of respiratory failure by either 'oxygenation failure' or 'ventilation failure.' In the meanwhile, technically speaking, respiratory failure type III occurs during perioperative periods that can be related to cardiopulmonary ECMO indications, to name a few, of "bridge to lung transplantation" [3, 4]; while respiratory failure type IV results from shock, which can be related to "myocardial infraction-association cardiogenic shock" [3, 4]. Nonetheless, for more focused investigation, this study condenses to the mortality of hypoxemic (type I: oxygenation failure) and hypercapnic (type II: ventilation failure) respiratory failure.
Although we are aware of the fact that other ECMO meta-analyses conducted database searches on PubMed, EMBASE, Cochrane, and so forth, we searched against the PubMed database only [38], due to the following reasons. During the pilot study, we found that this study required quite an inclusive search of keywords, as manifested by the total number of articles we worked with. In addition, unlike meta-analyses on relative risks and mean differences, a full-text was laboriously required to confidently make a decision to exclude its corresponding article, because the survival analysis is usually not the main topic of the referenced study but typically comprising just one line of hazard ratio information in the result table or one Kaplan-Meier survival curve figure. Nonetheless, we acknowledge that the risk of missing appropriate articles by not searching against multiple databases could have lowered the reliability of our study [39].
Whenever HRs and their variances were not reported explicitly, we estimated them from the information reported in the studies. Therefore, the significance of the results of the forest plot should have been diminished by our estimates of HR and variances. In further research, reporting numerical hazard ratios explicitly to facilitate later meta-analysis should be encouraged to investigate the mortality associated with ECMO use.
Based on the time-to-event data of respiratory failure, ECMO comprising both VV and VA types and the VV type alone has shown to provide advantages over alternative therapy. Although VV-ECMO alone on respiratory failure was mainly addressed in this study, future investigation of the efficacy of VA-ECMO alone in respiratory failure may be more informative, due to being a more common modality of ECMO yet with greater complications [5]. The accumulation of ECMO time-to-event data studies in respiratory failure will enable more focused mortality assessments, for example, on ARDS, exclusively.
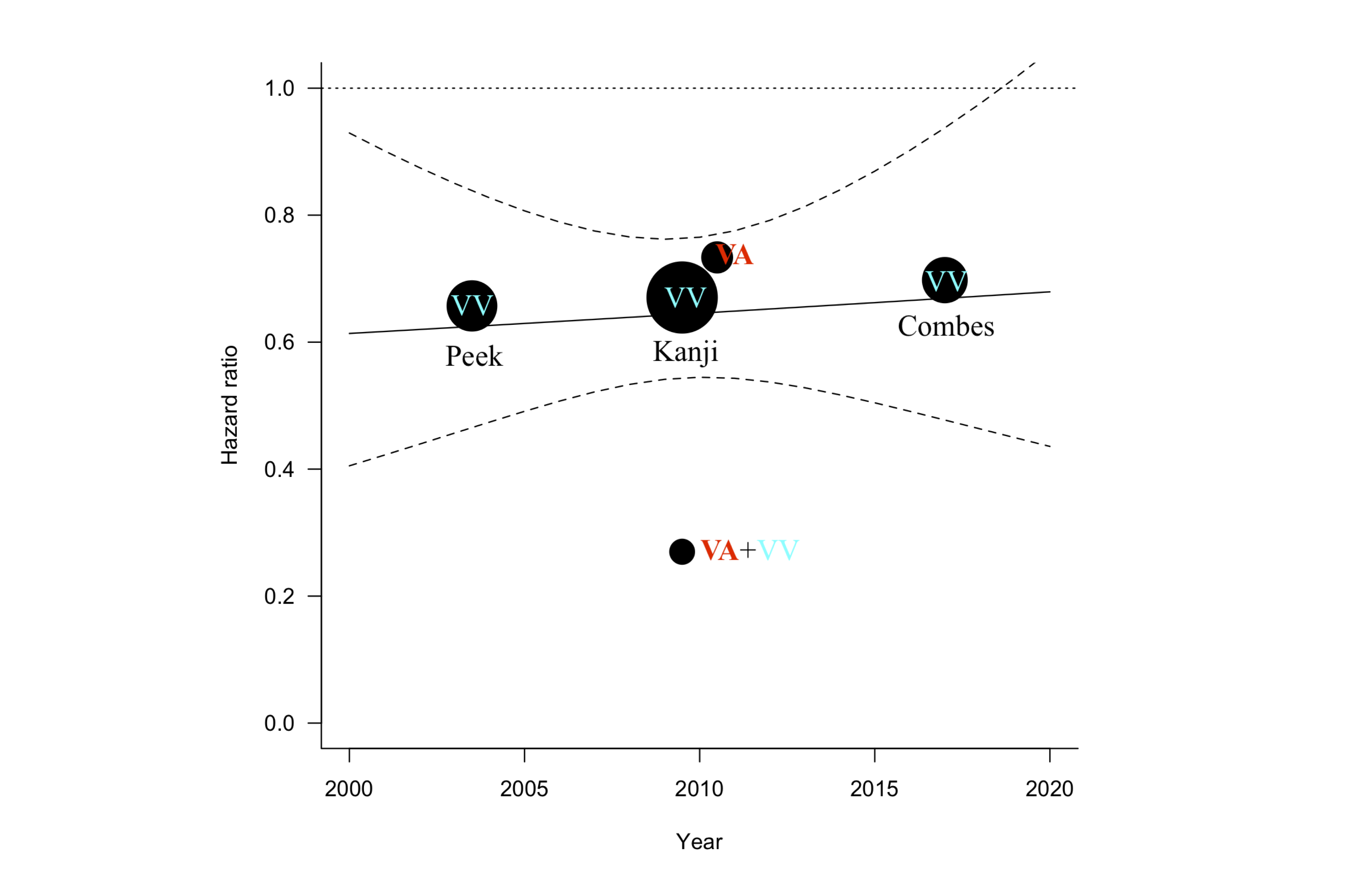
It is acknowledged that the ECMO technology from 1975 has changed immensely such that mortality may be correlated with the year, which is exemplified in the improved mortality over years in-between 1995 - 2000 and 2001 - 2004 [32]. For the referenced studies, the meta-regression analysis of the midpoint of the study period versus the hazard ratio (Figure 5) illustrates an insignificance (p-value = 0.8011) and neither positive nor negative correlation (r = 0.0635) in the scope of this study.
My Thoughts about Relevant Books, Films, and Media
Artificial Intelligence
In Ethem Alpaydin's "Machine Learning," while machine learning enables systems to adapt and learn from data in dynamic environments, artificial intelligence encompasses the broader capacity for systems to perform tasks requiring human-like intelligence, including but not limited to learning.
- A Perspective from 'AI Assistants' by Roberto Pieraccini
Deep Learning's Impact on Speech Recognition and Understanding: The evolution of machine learning, as detailed in "AI Assistants" by Roberto Pieraccini, particularly through deep learning, has fundamentally altered the approach to creating machine intelligence, transitioning from constructing complex programs to enabling machines to learn from examples. This shift has markedly enhanced the capabilities of machines in understanding and generating speech, with automatic speech recognition (ASR) and natural language understanding (NLU) seeing significant advancements. The advent of deep neural networks (DNNs) has led to the development of systems that can process speech and language in an end-to-end manner, obviating the need to optimize individual components separately. This holistic approach has not only streamlined the process but also resulted in synthetic speech nearly indistinguishable from human speech and performance levels previously unimaginable. Deep learning's role in these advancements underscores its singular effectiveness, outpacing traditional methods and embodying the new mainstream in crafting machine intelligence.
Divinity in Recommendation History: Recommendation engines are pivotal in shaping human decisions, much like the steam engine revolutionized the industrial age. The lineage of recommendation systems is intertwined with humanity's quest for wisdom and self-reflection. Historically, these systems were seen as divine conduits, with oracles and astrologers in ancient civilizations like Greece, China, and Rome offering insights into life's dilemmas. The I Ching, for instance, stands as a primeval algorithmic system, compensating its lack of personal data with a rich, evocative user experience. Despite the shift from divine to data-driven systems over millennia, the human yearning for guidance remains unaltered, underscoring our continuous search for meaningful advice and self-discovery.
Singular Value Decomposition (SVD): In the realm of recommendation engines, Singular Value Decomposition (SVD) plays a crucial role. This mathematical technique reduces data to its most informative elements, uncovering 'latent features' that influence user preferences. By breaking down complex matrices into simpler submatrices, SVD reveals hidden connections and similarities between users' tastes, transcending the limitations of traditional nearest neighbor methods. It's a profound tool that can identify shared preferences even among users with no direct rating overlaps, demonstrating the depth and complexity of modern recommendation systems.
Reward Function to Navigate AI Decision-Making Complexity: In the realm of artificial intelligence, the reward function emerges as a critical component in navigating the inherent uncertainties of decision-making with finite, incomplete data. This function enables AI to probabilistically model and pursue actions that maximize expected rewards, regardless of the environment's complexity. Such a mechanism is vital for AI to effectively address a broad spectrum of challenges, including the basic need for resources, illustrating its role in adapting to any given situation with the most advantageous strategy. The true measure of AI, however, lies not in its ability to mimic human emotions but in its consistent behavior towards achieving long-term, desirable outcomes. Designing a reward function that ensures such behavior, while preventing undesirable actions, presents a significant challenge, underscoring the delicate balance between maximizing efficiency and adhering to ethical standards. Ultimately, the effectiveness and safety of AI hinge on the careful crafting of reward functions that can handle the unpredictability of real-world scenarios without faltering.
AI-Complete: Tasks that necessitate human-level intelligence for resolution, signifying an AI system's attainment of general intelligence on par with humans, are known as AI-complete challenges. These tasks often involve complex decision-making and understanding, akin to roles such as lawyers, scientists, and psychiatrists. Successfully performing AI-complete tasks means the AI can reason, plan, learn, and comprehend natural language at a level currently unique to humans, marking a significant milestone in AI development. Understanding AI-complete challenges helps grasp the scope of AI's potential and the innovation needed to attain human-like intelligence.
Intuition Unchained: Peter J. Denning and Matti Tedre, in "Computational Thinking," highlight a transformative trend within mathematics and logic with their observation: "[M]uch work in mathematics and logic has aimed at eliminating intuition from routine calculation and logical inference. Eliminating intuition from routine jobs did not mean eliminating experts, but rather making their expertise available to a large number of non-expert people." This perspective emphasizes not the obsolescence of human intuition in the wake of artificial intelligence (AI) but the augmentation of human capability, where AI serves as a bridge, enabling non-experts to advance step by step in tasks traditionally necessitating intuition.
The integration of AI into various domains does not supplant the need for human intuition; instead, it amplifies the potential for collaborative problem-solving, where intuition and computational power converge. This synergy allows for the broadening of expertise beyond traditional confines, empowering those without specialized knowledge to engage meaningfully with complex tasks. In essence, AI acts not as a replacement for intuitive human processes but as an enhancer of human intellectual endeavors. This nuanced approach heralds an era where innovation is not solely the domain of the expert but is accessible to a wider audience, facilitated by AI's ability to democratize the process of discovery and decision-making.
Hannun et al. published an article in Nature Medicine in 2019 that demonstrated how a deep neural network (DNN) could outperform cardiologists in the diagnosis of 14 different heart arrhythmias using ECG data. The DNN was trained on a dataset of over 400,000 ECG recordings and achieved an accuracy of 94.4%, compared to an average accuracy of 80.6% for a group of cardiologists. The study suggests that DNNs could potentially be used as a diagnostic tool for arrhythmias, and may even outperform human experts in some cases.
- A.I. Engine
ChatGPT, developed by OpenAI, marks a pivotal moment in AI, often compared to the "iPhone moment" in smartphones. This analogy draws from the iPhone's transformative impact on mobile technology, as emphasized by Steve Jobs in 2007 (Apple Inc., 2007).
- In-Database Machine Learning
The traditional approach to database processing often involves significant resource expenditure in moving data to and from algorithms, which can be a bottleneck. In-database machine learning, however, represents a paradigm shift by integrating the machine learning algorithms directly within the database engine, accessible via SQL. This approach eliminates the need for moving data, thereby offering faster performance and enhanced security. Apache Hadoop is a prime example of this innovation, as it offers a comprehensive suite of tools including Hadoop MapReduce, which collectively enable efficient in-database processing and analysis of large data sets.
- Exploring AI raises profound questions about our knowledge, society, and ethics, across several key domains:
Post-humanism: Post-humanism challenges the idea that AI must mimic human intelligence or morality. It suggests that AI might develop distinct forms of intelligence and moral reasoning, different from human capabilities. This raises questions about the moral capacities and responsibilities of AI systems, especially when they make decisions with ethical implications, like in the case of self-driving cars facing moral dilemmas. The debate extends to how interacting with AI affects human morality, examining our actions towards AI through the lens of our own moral character.
Totalitarianism: The concern with AI in the context of totalitarianism revolves around its potential use in subtle forms of manipulation and surveillance. This is not limited to overtly authoritarian political systems but can manifest in everyday technologies, like children's toys embedded with AI. These devices, while seemingly innocuous, may collect and utilize personal data without the user's knowledge, leading to privacy concerns and the potential misuse of information. This scenario exemplifies the hidden yet effective ways AI can be employed in monitoring and influencing behavior, raising ethical questions about consent and data security.
Responsibility in Relation to Transparency and Explainability: As AI gains more autonomy in tasks traditionally done by humans, assigning moral responsibility becomes complex. AI's decisions, often fast and based on intricate algorithms, challenge our ability to intervene or fully understand their rationale. This leads to the "black box" problem, where the AI's decision-making process is not transparent, especially in advanced systems like deep learning. While decision trees are more transparent, deep learning algorithms can be opaque, leaving users and creators uncertain about how decisions are made and their consequences. Thus, even with AI's increasing capabilities, the question of who bears responsibility for its actions remains a significant ethical challenge.
Singularity & Transhumanism: The concept of Singularity — where AI may surpass human intelligence and potentially merge with it — raises concerns about our readiness to address the ethical and societal implications of such advanced systems. This ties into transhumanism, the idea of enhancing human abilities and longevity, possibly leading to a new form of existence, as explored by Yuval Noah Harari in "Homo Deus." The rapid development and application of such technologies might outpace our understanding of their broader consequences.
↓ This content is not sourced from the book "AI Ethics." ↓
In the United States, the foundation for much of the nation's privacy legislation is rooted in the Fair Information Practice Principles established in 1973. These principles have significantly influenced the country's approach to privacy law. In the European Union, initial steps towards privacy legislation were taken with the Data Protection Directive in 1995, which set the groundwork for privacy regulations in the EU. This was further expanded by the General Data Protection Regulation (GDPR) in 2016, which built upon the Data Protection Directive's principles, offering comprehensive and enforceable data protection standards across all EU member states.
However, a more universally acknowledged framework for personal privacy and data protection is found in the Organisation for Economic Co-operation and Development (OECD) Guidelines on the Protection of Privacy and Transborder Flows of Personal Data, first published in 1980. These guidelines provide a clear definition of personal data, referring to it as records related to an identifiable individual, known as the data subject. The OECD guidelines in 2013 lay out eight core principles designed to safeguard the privacy of data subjects:
Collection Limitation: Personal data collection should be restricted and conducted lawfully and fairly. Where possible, it should be done with the data subject's knowledge or consent.
Data Quality: Data must be pertinent to its intended use and maintained accurately, completely, and up-to-date as necessary.
Purpose Specification: The reasons for collecting personal data should be clearly defined at the time of collection. Use of the data should be confined to these specified purposes or those compatible with them, with any change of purpose explicitly stated.
Use Limitation: Personal data should not be used or disclosed for purposes other than those specified, except with the subject's consent or under the authority of law.
Security Safeguards: Reasonable security measures must be in place to protect personal data from risks like loss, unauthorized access, or misuse.
Openness: There should be a policy of transparency regarding practices and policies related to personal data. Information about data collection and usage, as well as details about the data controller, should be easily accessible.
Individual Participation: Individuals should have the right to confirm if a data controller has their personal data, access their data in a timely and reasonable manner, and challenge or appeal any refusal to grant access. They should also be able to contest the accuracy of their data and have it corrected or amended as needed.
Accountability: Data controllers must be accountable for adhering to these principles, ensuring compliance with the appropriate measures.
Federated Learning is particularly relevant in scenarios involving multiple healthcare institutions. It is a decentralized form of data processing, ideal when dealing with diverse and widespread data sources, such as several hospitals contributing to a joint research study. In this setup, each hospital trains a local model on its own data and then sends only the model updates, not the raw data, to a central system. These updates are then aggregated to improve the overall model. This method ensures that the core model benefits from the diverse data while maintaining the confidentiality of individual patient records, as the actual data remains within the confines of its original location.
Differential Privacy is a method that ensures the privacy of an individual's data in analyses by guaranteeing that results do not hinge on any single person's information. The methodology is strengthened by adding randomness to the data, either through techniques like a randomized coin flip or by applying the principles of the Laplace distribution to adjust the sensitivity. This introduction of noise effectively masks individual data points, thus significantly enhancing privacy and security in the data analysis process.
- A Perspective from 'AI Assistants' by Roberto Pieraccini on the Impact of GDPR and Federated Learning
The Role of GDPR in Shaping Digital Privacy: In the evolving landscape of digital privacy, the General Data Protection Regulation (GDPR) stands as a cornerstone of privacy protection within the European Union, underscoring the significant shifts required by industries to align with stringent data handling and privacy standards. Enacted in 2016, GDPR has spurred a reevaluation of how personal data is collected, processed, and stored, emphasizing the importance of user consent, data minimization, and the safeguarding of personal information against unauthorized access. This regulatory framework has catalyzed a move towards more secure and privacy-preserving methodologies in the development and deployment of machine learning (ML) technologies, reflecting a broader awareness of privacy risks in the digital domain, including social networks, smart home devices, and virtual assistants.
Federated Learning - A Paradigm Shift in Privacy-Preserving Technology: Amidst this backdrop, federated learning emerges as a pioneering approach, exemplifying the shift towards privacy-centric technology development. Conceived by Google, federated learning enables ML models to learn from decentralized data sources without the need to transfer personal data to the cloud. This model of computation is particularly beneficial for applications requiring sensitive data processing, such as speech recognition or text input on mobile devices, allowing for continual improvement of local model performance through ML training directly on the device. By leveraging the increasingly powerful computing capabilities of personal devices, federated learning ensures that personal data remains within the user's control, with only encrypted, aggregated updates shared to refine and enhance the collective intelligence of the system. This not only safeguards user privacy by design but also signifies a significant advancement in the utilization of ML for personalization and efficiency, without compromising data security.
- A Perspective from 'Deep Learning' by John D. Kelleher on Privacy and Ethics in Algorithmic Decision-Making
The increasing reliance on algorithmic decision-making, particularly in deep learning, raises significant privacy and ethical concerns. Recital 71 of the General Data Protection Regulation (GDPR) emphasizes the necessity of transparency by affirming that individuals affected by automated decision-making processes have the right to understand how these decisions are made. However, the legal clarity of this "right to explanation" remains ambiguous, with specific implications for machine learning and deep learning still to be fully defined through judicial interpretation. This ambiguity underscores the societal need for a better understanding of how deep learning models use personal data. From a technical perspective, the ability to interpret and analyze the inner workings of these models is crucial, as it can reveal biases and pinpoint scenarios where the model may fail. In response, the AI research community is increasingly focused on explainable AI, with numerous projects and conferences dedicated to enhancing transparency and human interpretability in machine learning. By analyzing the inputs that trigger specific behaviors in a network, such as neuron activation, researchers can improve the transparency of AI systems, ensuring their alignment with GDPR requirements and broader ethical standards. This emphasis on explainability and accountability aims to address the ethical and privacy concerns associated with algorithmic decision-making, fostering more responsible and trustworthy AI systems.
Virtual Reality (VR): VR immerses users in entirely fictional yet realistic virtual environments, isolating them from the physical world. It provides a complete escape into computer-generated scenarios, often with a sense of presence and interaction.
Augmented Reality (AR): AR enhances our real-world experience by overlaying convincing digital images, sensory elements, and haptic feedback onto our physical surroundings. It allows users to interact with digital information while remaining in the physical world.
Mixed Reality (MR): MR blends real and virtual elements seamlessly, enhancing our perception and interaction with our surroundings. It overlays virtual or augmented features onto the real world, creating a unified and immersive experience.
Extended Reality (XR): XR is a transformative realm that encompasses various immersive technologies, with Virtual Reality (VR) offering complete immersion and Augmented Reality (AR) complementing the physical world. When VR and AR converge into Mixed Reality (MR), it marks the dawn of XR's potential. What sets XR apart is its profound ability to bridge the gap between humans and computers. Our brains are inherently wired to perceive events in 3D, and XR takes this connection to the next level. XR's promise lies in its potential to create immersive, interactive, and multisensory environments, empowering professionals to control and adapt their surroundings while leveraging real-time feedback. In this evolving landscape, augmented, virtual, and mixed realities redefine perception, offering innovative ways to interact with the world. Yet, realizing XR's full potential hinges on the sophisticated integration of digital technologies and software capable of orchestrating seamless virtual experiences.
- Challenges and Solutions in Extended Reality (XR)
Challenges in Extended Reality (XR): Overcoming the hurdles in the realm of Extended Reality (XR) is no small task. Ensuring that results like data overlays or graphic representations are visible in real-time is crucial, as even the slightest lag can disrupt the immersive Augmented Reality (AR) experience. Additionally, integrating haptic feedback into devices such as smartphones and game controllers is a distinct challenge, as it demands precision and realism, not merely a general approximation of touch. Moreover, the stakes are high in AR systems, especially when used in hazardous work environments; rendering images or data inaccurately could lead to serious injuries or even fatalities. What makes XR design and engineering particularly challenging is the vulnerability to even the tiniest glitches or flaws in hardware, software, user interfaces, or network performance, which can swiftly transform a convincing XR environment into an implausible one.
Balancing Realism and Comfort in XR Environments: While there's a common notion that virtual reality and other XR forms must replicate reality flawlessly, this belief isn't always necessary. In many cases, the objective is to create environments realistic enough to elicit desired responses in the mind and body without aiming for absolute fidelity. To strike a balance, those designing and developing XR frameworks must navigate trade-offs between fidelity and immediacy. Within virtual worlds, the creation of the illusion of events, while avoiding sensory overload from genuine physical forces and motions, becomes a priority. Embracing a muted experience can reduce sensory conflicts that often lead to discomfort, dizziness, or motion sickness within virtual environments. Moreover, duplicating the exact physiology of the hand isn't imperative; the goal is to trick the brain into perceiving a realistic sense of touch, not replicating every intricate detail.
↓ In resonance with the themes explored in Samuel Greengard's book 'Virtual Reality,' this discussion presents my independent insights and perspective. ↓
- Exploring the Synergy of 3D Glasses, XR, and Hinduism in 'Avatar'
Spatial Realization through 3D Glasses: In James Cameron's "Avatar," the introduction of 3D glasses wasn't coincidental but aligned perfectly with the core principles of Extended Reality (XR). These glasses enhance three-dimensional perception, a vital component for immersive XR experiences. The film portrays Jake Sully, a disabled character, who undergoes a profound transformation as he enters the world of the Na'vi, utilizing an Avatar that allows him to seamlessly perceive and interact with his new Na'vi body. This spatial realization experienced by the audience, made possible by 3D glasses, not only harmonizes with XR concepts but also beautifully mirrors Jake's journey of self-discovery and transformation throughout the narrative.
The Hinduistic Concept of Avatar in XR: Additionally, the film's exploration of the Hindu concept of avatar, where individuals take on new forms for a purpose or to bring about change, adds depth to its narrative. Jake's transition into his Na'vi Avatar can be seen as a metaphorical representation of the Hindu avatar concept, emphasizing the film's exploration of identity and transformation within the context of XR technology. The synergy between 3D spatial perception and the Hinduistic concept of avatar underscores the film's exploration of XR's transformative power and its ability to explore complex themes of identity, spirituality, and the blending of reality and fiction.
- 'Ready Player One' and the Inspiration Behind VR Innovation
The VR Landscape of 'Ready Player One': In 'Ready Player One,' the depiction of technology within the OASIS primarily aligns with the principles of virtual reality rather than the broader spectrum of extended reality. This distinction is evident in the complete immersion of users into a fully digital universe, where the physical world is entirely obscured in favor of a computer-generated environment. The use of immersive VR gear, which includes headsets and haptic suits, enables users to interact with and experience the OASIS as an entirely separate reality. Unlike XR, which includes augmented reality (AR) and mixed reality (MR) to blend or augment the physical world with digital elements, the VR in 'Ready Player One' is characterized by its exclusive focus on creating a separate virtual experience. This emphasis on VR as a form of total escapism and transformative potential of entirely immersive digital worlds is underscored by the poignant reminder from James Halliday, the creator of the OASIS, that "Reality is the only thing that's real." This statement reinforces the film's depiction of VR, underscoring a clear demarcation from XR by highlighting the importance of distinguishing between virtual escapism and the tangible, irreplaceable value of real-world experiences.
How 'Ready Player One' Prefigures XR Developments: Despite the visual similarities between the VR goggles depicted in the movie and the Apple VisionPro, the latter is designed for extended reality (XR), offering capabilities beyond the VR-specific focus showcased in the film. The movie's emphasis on VR technologies, such as haptic suits and immersive visors, mirrors current technological trends and underscores the importance of tactile feedback and facial recognition in enriching virtual experiences.
- The Matrix: VR and the Realm of Simulated Reality
VR and Beyond: "The Matrix" franchise, while not explicitly categorized under contemporary terms like AR (Augmented Reality), XR (Extended Reality), or VR (Virtual Reality), significantly explores concepts that are foundational to these technologies. The films depict a dystopian future where humanity is unknowingly trapped in a simulated reality called the Matrix, created by sentient machines. This simulated reality is so comprehensive and immersive that it effectively functions as a form of virtual reality, albeit one that individuals are forcibly plugged into without their knowledge or consent. The Matrix's simulated world parallels VR in that it's a completely immersive digital environment where physical laws can be bent or broken, and individuals interact within this space as if it were the physical world. However, it goes beyond traditional VR because it's not a voluntary or leisure activity; instead, it's a pervasive illusion meant to subdue humanity. While "The Matrix" doesn't explore AR or XR in the sense of overlaying digital information onto the real world or blending real and virtual environments in a seamless manner, its exploration of virtual reality's philosophical and ethical implications has profoundly influenced public perception of VR and related technologies.
- Exploring AR and MR Technologies in 'Minority Report'
Precognitive Visions and Advanced Technologies: In "Minority Report," the use of Augmented Reality (AR) and Mixed Reality (MR) technologies is further exemplified through the innovative depiction of precognitive visions — the futuristic images seen and recorded by the three precogs. These visions, central to the film's plot, are integrated into the physical environment of the PreCrime unit, where law enforcement officers can interact with and analyze these future events in real time.
Through the Lens of AR: AR is demonstrated through the overlay of these precognitive visions onto physical screens and interfaces within the PreCrime headquarters. This allows them to examine details of potential crimes before they occur, enhancing their ability to prevent them. The seamless integration of digital information (the precogs' visions) into the physical workspace exemplifies AR's capability to augment reality with additional layers of data.
Exploring MR's Potential: MR is showcased as these holographic images are not just passively displayed but are interacted with through gesture-based controls. The protagonist, John Anderton, uses hand gestures to move, scale, and probe into the holographic data, merging digital and physical realities. The MR technology enables a more immersive interaction with the digital content, allowing Anderton and his team to explore the visions spatially as if they were physically present within the scene of the future crime. This blending of real and virtual elements is a hallmark of MR, creating an environment where digital and physical worlds coexist and interact in real time.
- Tron: The 1982 Odyssey into Digital Universes and the Dawn of Virtual Gaming
Game On in VR: The 1982 film Tron pioneers the depiction of an intricate digital universe within a computer system, setting a foundational narrative for the interaction between humans and digital realms. This visionary work presages the immersive digital spaces that are central to contemporary VR discussions. Remarkably, the film emphasizes the significance of gaming, a concept that, while universally acknowledged today, was groundbreaking in 1982. Flynn not only highlights the crucial role of gaming in the real world, attributing it substantial value in terms of corporate power and financial gain, but also extends this importance into the virtual realm. It presents a narrative where the protagonist, absorbed into the game's universe, must navigate its challenges to unearth evidence of corporate malfeasance — specifically, the theft of a game by Dillinger from Flynn.
- The Convergence of VR and Reality in 'Tron: Legacy'
From VR to Reality: "Tron: Legacy" explores the dynamic relationship between Virtual Reality (VR) and its implications in the real world, building on the foundational themes introduced in the 1982 classic, "Tron." This sequel makes the intricate concepts of computer science more digestible and engaging for audiences, particularly those with a prior understanding of the original film's universe. It articulates the digital domain's potential to address critical real-world issues, notably highlighting (1) VR's significant role in tackling global challenges like disease control and prevention, while also considering (2) the possible dangers these technologies may introduce to the real world. (1') Central to this narrative is the concept of ISOs (Isomorphic Algorithms), which represent a breakthrough in digital evolution with the potential to bring about revolutionary changes in technology and science. The character of Quorra, an ISO, symbolizes the key to unlocking these transformative advancements. (2') Meanwhile, the antagonist Clu, a digital replication of Flynn (the protagonist's father), aims to destroy the ISOs and extend his dominion to the real world by leveraging an army from within the VR landscape. This conflict underlines the ethical and existential questions that arise from advancements in digital technology. The story elegantly weaves together the optimistic prospects of VR and the pioneering spirit of the ISOs with a cautionary narrative about the disruptive potential of technology, showcasing the intricate interplay between virtual innovations and their tangible impacts on the real world.
Cinematic Foresight: In "Tron: Legacy," the intertwining of digital and physical realities is not just a flight of cinematic imagination but a foretelling of the IoT and digital twin technologies discussed in Samuel Greengard's book, "The Internet of Things." This body of work reveals how such innovations, much like in the film, create precise virtual counterparts of physical systems, enabling profound insights and simulations. It underscores how today's use of these technologies, from NASA's spacecraft design to architectural pre-construction VR walkthroughs, mirrors the movie's portrayal of VR's deep-seated impact on the tangible world. The narrative's vision presented in "Tron: Legacy" of virtuality reshaping real-world challenges has emerged into reality, confirming that the film's previously speculative ideas have transitioned into tangible components of our contemporary technological advancements.
- From BOTW to TOTK: The Impact of 'The Legend of Zelda' on VR Gaming
"The Legend of Zelda: Breath of the Wild" (BOTW) and its sequel, "Tears of the Kingdom" (TOTK), stand as monumental achievements in the evolution of virtual reality (VR), presenting a detailed exploration of memory, identity, and the deep connections that bind characters across time. BOTW introduced players to a vast open-world adventure, pioneering in its VR capabilities and narrative depth, where the protagonist Link embarks on a journey of self-discovery through the fragments of his past memories. This exploration shares thematic resonance with iconic films like "Ghost in the Shell" and "Blade Runner," where the core narrative revolves around the pivotal role of memories in defining one's identity.
TOTK further expands this narrative framework, exploring the ancestral ties and the very essence of Hyrule's history. (1) The nuanced portrayal of Zelda in TOTK, particularly her transformation into a light dragon to heal the Master Sword, not only cements her central role in the saga but also justifies the series' title, 'The Legend of Zelda.' The act of self-sacrifice, transforming into a light dragon to empower and heal the Master Sword over many generations, alongside the sword's restoration, is what truly defines the Legend of Hyrule. (2) Moreover, Link's role in connecting different eras — awakening after 100 years to confront calamity in BOTW, and in TOTK, using the ancestral Rauru's hand to access memories within the tears of the Light Dragon, thereby understanding past events to determine his actions — illustrates the very reason he is named "Link." This naming reflects his unique ability to bridge past and present, embodying the essence of connectivity and continuity, not just as a focus of the series but as a fundamental characteristic of his identity and purpose within the saga.
Through these intricate narratives, both BOTW and TOTK have effectively elevated the gaming community's perception of VR's capabilities, transcending traditional gameplay to explore complex themes of memory, identity, and legacy. By intertwining the fates of Zelda and Link with the fabric of Hyrule itself, these games not only redefine the potential of virtual storytelling but also affirm why the saga rightly celebrates Zelda's legend, embodying a transformative experience that bridges multiple generations and narratives within the immersive realms of virtual reality.
- My Reflections on 'Spatial Computing': Shaping the Future of Healthcare and Mixed Reality
In "Spatial Computing" by Shashi Shekhar and Pamela Vold, the authors present a future where "all software needs to be spatially aware and where every user is a participant in updating the location information presented with that software." This vision highlights the transformative potential of spatial computing across various domains, including mixed reality (MR) and healthcare. By leveraging spatially aware software, MR applications can enhance the physical world with digital augmentations, leading to more immersive educational and therapeutic experiences. In healthcare, this technology allows professionals to interact with dynamic, three-dimensional representations of patient anatomy, improving diagnostics and surgical precision. The analogy of a baby monitor as a remote-sensing system underscores the practicality and impact of spatial computing, illustrating how everyday objects can gather and utilize spatial data. This participatory, dynamic approach to data not only advances the capabilities of MR and healthcare but also signals a shift towards more personalized, efficient, and interactive technologies.
Regardless of the industry, there's a need for a more flexible and expansive approach to intellectual property than previous generations adopted. Intellectual property laws are undergoing rapid transformations globally, affecting copyrights, patents, and trademarks alike. The most significant shifts are evident in the strategic thinking of business leaders regarding intellectual property, showcasing a dramatic evolution in just the last ten to twenty years.
Intellectual property fundamentally comprises information, its value often rising with increased usage rather than diminishing. Even without monetizing access, organizations can derive substantial benefits when others utilize their created information, as observed with MIT's asset value surge following the OpenCourseWare platform's launch. This instance exemplifies how relinquishing tight control over intellectual property, particularly patents and copyrights, can enhance its worth. Consequently, adopting a balanced strategy encompassing sharing, licensing, and potential charging for intellectual property utilization could optimize value creation for the organization.
Entering a co-development agreement with another organization presents a viable strategy for acquiring intellectual property, a practice prevalent in certain industries but applicable across various economic sectors. Such agreements facilitate collaborative intellectual property development, incorporating a "covenant not to sue," ensuring legal protection during the partnership. When executed effectively, both parties stand to gain increased profits, market share, and enhancements to their intellectual property portfolios. This arrangement ensures joint ownership of any interoperability technology developed together, enabling organizations, regardless of whether they are competitors or operate in complementary domains, to expand their intellectual property portfolios beyond the capabilities of their internal staff.
- A Paradigm Shift in Collaborative Development (in the Web 2.0 Era)
A crucial aspect of the recent surge in Web development, known as Web 2.0, is the trend of companies opening up their systems for interoperability with external developments. The most remarkable growth in the Internet and mobile communications sector is now propelled by collaborative development between customers, third parties, and major software corporations like Facebook and Apple. Apple, for instance, has ingeniously engaged iPhone users and the broader developer community through the iPhone Development Center, fostering the creation of applications across its devices.
This trend is encapsulated in the Open Application Programming Interfaces (Open API) movement, where various participants contribute to a widely accessible ecosystem for developing, using, and refining computer applications, along with managing the data flow between them. Open innovation, the underlying principle of this movement, is straightforward yet potent: innovation can stem from outside your organization. Historically, businesses hesitated to embrace external ideas, partly due to fears of potential compensation claims. However, the desire for improvement and the pleasure derived from creation drive many customers to contribute, demonstrating a central lesson from the Web 2.0 and user-generated content phenomena.
While individuals partake in this process out of self-interest, they also seek enhanced products, believing they can offer better solutions. Open innovation allows organizations to tap into this pool of ideas, necessitating discernment in selecting and incorporating valuable suggestions. This strategy, while maintaining organizational control, can lead to substantial product and service enhancements and even entirely new offerings.
Google and its subsidiary YouTube exemplify this trend. Google distinguishes itself through its proprietary intellectual property, crucial for its search engine dominance. However, its existence relies heavily on the copyrighted material available worldwide on the web. Similarly, YouTube doesn't create its own copyrighted video content but provides a platform for users to share video and audio content, showcasing the symbiotic relationship between major platforms and user-generated content.
↓ In alignment with the concepts explored in 'Intellectual Property Strategy', the following discussion offers my own independent insights and a perspective that resonates with the themes of the book. ↓
- Navigating the Digital Evolution From Web 1.0 to 4.0
In "Cybersecurity" by Duane C. Wilson, the evolution of the World Wide Web (WWW) since its inception by Tim Berners-Lee in 1989 is concisely outlined through its generational shifts. Web 1.0 served as an information portal for businesses, marking the web's initial phase as a broadcast medium. The emergence of Web 2.0 introduced the concept of social networking, grouping individuals by shared interests and enabling a more interactive experience.
Web 3.0 (or the semantic web): Web 3.0 represented a significant leap towards making the web more intelligent, with an emphasis on machine-readable content. This era focused on reducing human tasks by enabling machines to understand data relationships, integrating artificial intelligence (AI) and machine learning (ML) to process and analyze data efficiently.
Web 4.0 (or the symbiotic web): Web 4.0 advances this interactivity, allowing machines to operate autonomously in response to internet content, such as recalling a user's last viewed page or tailoring ads to past searches. This creates a more intuitive and personalized web experience, highlighting a deeper symbiosis between humans and machines.
- IP Strategy for the Symbiotic Web Era (Web 4.0): A Personal Perspective
Crafting IP Strategies for Web 4.0: The intellectual property (IP) strategy for Web 4.0, often characterized as the Symbiotic Web, necessitates a forward-thinking, adaptive approach that recognizes the intricate interactions between humans, machines, and data. Web 4.0 introduced new challenges and opportunities for managing IP.
Adaptive IP Strategy for AI Innovations: In the constantly evolving environment of Web 4.0, where AI and machine learning are at the forefront of content creation and innovation, the need for a flexible intellectual property (IP) strategy becomes apparent. This approach calls for a thoughtful update to IP laws to better define the ownership of AI-generated content, exploring how such creations can be protected, and pondering over who should be considered the rightful IP owner — be it the AI developer, the user, or perhaps, in a more speculative sense, the AI itself. I'm particularly intrigued by how IP will be defined for AI-generated innovations. This scenario underlines the importance of agility in IP management, encouraging companies to quickly adjust to new technological advancements by securing patents, trademarks, and copyrights for emerging innovations. Such a proactive and reflective stance ensures that IP strategies can keep pace with the digital transformation, safeguarding breakthroughs and fostering the swift progress characteristic of Web 4.0.
- The Impact of Creative Priorities on Artistic Work and IP Strategies in the Digital Age: A Personal Perspective
- Balancing Open Innovation and Strategic Protection: A Personal Perspective
The expiration of key patents, such as LEGO's 1958 patent for its unique brick design, has led to a surge of LEGO-compatible products and imitation brands, diversifying the market with more affordable interlocking bricks and a wider range of themes and models. Similarly, the looming expiration of copyrights like Walt Disney's Mickey Mouse indicates a decline in monopolistic control, heralding a new era of artistic freedom and a richer cultural landscape. However, this doesn't mark a complete end to exclusivity; companies like LEGO and Walt Disney are continually filing new patents to maintain their competitive edge, even as their older patents expire. This balance between the end of certain exclusive rights and the pursuit of new ones by these corporations facilitates both the sustenance of their market dominance and the flourishing of creativity and innovation in the public domain.
Why Cloud Computing?: Cloud computing represents a paradigm shift from traditional capital expenditure (CapEx) models, which necessitate significant upfront investment in hardware, to operating expense (OpEx) models that allow for payment based solely on consumption. This model facilitates substantial cost savings and enhances flexibility by enabling the reuse of computing resources and functions, thereby contradicting Gossen's First Law of diminishing returns. In the realm of cloud computing, the utilization of these resources can actually lead to increased value over time, offering an inverse relationship to Gossen's principle. By allowing for the rapid deployment of pre-existing functionalities, businesses achieve greater agility and a reduced time to market for their products and services. Essentially, cloud computing turns the traditional economic model on its head, demonstrating that, unlike the typical diminishing returns seen in other areas, the strategic use of cloud services can amplify efficiencies and benefits with each use.
NIST's Definition: Cloud computing, as defined by NIST (National Institute of Standards and Technology), is a model that provides widespread, easy, and immediate access to a collective pool of configurable computing resources, enabling them to be quickly allocated and released with minimal effort from management or interaction with the service provider. This model is designed to ensure high availability and comprises five key characteristics: broad network access, on-demand self-service, pooled resources with virtualization, rapid scalability, and services measured and metered for use. It is structured around three core service models — Infrastructure as a Service (IaaS), Platform as a Service (PaaS), and Software as a Service (SaaS) — and is deployed through four models: public, private, community, and hybrid clouds.
(1) Virtualization to (2) Cloud: Cloud computing and virtualization serve as cornerstone technologies in modern IT infrastructures, with (1) virtualization enabling multiple virtual environments to run on a single physical hardware system through server and application virtualization. VMware exemplifies server virtualization by dividing a physical server into multiple virtual servers, allowing for efficient resource distribution and coexistence of various operating systems on a single server, while application virtualization simplifies deployment by enabling centralized access for multiple users. In contrast, (2) cloud computing expands on virtualization's resource optimization, providing scalable, flexible, and metered computing services over the internet, such as servers, storage, and software. It introduces key features like on-demand self-service, broad network access, and rapid elasticity, distinguishing itself from virtualization by offering a comprehensive service model that includes infrastructure, platform, and software as services, thus facilitating a broader range of IT solutions beyond mere resource efficiency.
Unveiling Shadow IT: Shadow IT refers to the use of IT systems, applications, or services without the explicit approval of an organization's central IT department. This practice is particularly prevalent in cloud computing, where the ease of accessing and deploying cloud services enables individuals or departments to bypass traditional IT controls. While shadow IT can foster innovation by allowing users to quickly meet their needs, it also poses significant risks, including security vulnerabilities and compliance issues, due to the lack of oversight and integration with the organization's IT infrastructure. In the context of cloud computing, the unchecked use of shadow IT amplifies these challenges, potentially leading to data breaches and operational inefficiencies as organizations struggle to manage a sprawling, unsecured digital environment.
↓ The information provided does not originate from the book "Cloud Computing," but it has been supplemented with relevant information. ↓
- Privacy Enhanced Through the Power of On-Device AI in Mobile Devices
Samsung Galaxy S24's On-Device AI Revolution: Samsung Galaxy S24 Series introduces a groundbreaking shift towards enhancing user privacy with its advanced on-device AI capabilities. By processing data locally, this technology ensures that personal information remains secure within the device, eliminating the risk associated with external server storage and potential breaches. This move not only caters to the increasing consumer demand for privacy but also sets a new standard in the mobile industry by prioritizing the protection of user data amidst growing concerns over digital privacy.
Galaxy S24 vs. Cloud Vulnerabilities: Contrastingly, relying on cloud-based services for tasks such as translation exposes user data to risks, as it requires processing on external servers beyond the user's control. Despite the robust data protection measures employed by companies like OpenAI, the inherent vulnerability associated with transmitting and storing data off-device poses a significant privacy threat. The Galaxy S24 Series addresses these concerns by keeping all data, including personal conversations and documents, securely within the device, thus offering a superior level of privacy and security.
Paradox of IoT Dependence: At a pivotal point, the advancement of AI and IoT (Internet of Things) is transforming computers from mere reservoirs of human-inputted information into self-sufficient entities with the capacity to perceive the world autonomously, leading to an era where machine independence overshadows human skill. This seismic shift towards a deeply interconnected digital ecosystem offers remarkable insights and operational efficiencies but also posits a paradox; the very technology meant to augment human life could potentially erode fundamental knowledge and skills. If our reliance on technology becomes absolute, the absence of these smart systems could expose a vulnerability in our species, leaving us ill-prepared to manage basic survival tasks without digital assistance. This scenario underscores a profound concern: the advancement of AI and IoT, while propelling us forward, may also be leading us to a precipice where, stripped of these aids, we could find ourselves at a loss, disconnected not only from our roots but potentially jeopardizing our future as a species.
The Fourth Industrial Revolution (4IR) and the Industrial Internet of Things (IIoT): 4IR represents a fundamental shift in the industrial landscape, marked by the integration of cyber-physical systems that blend the physical and digital worlds. At the core of 4IR is IIoT, where machines embedded with smart sensors communicate and interact with each other, with humans, and across digital platforms. This evolution, building on the previous revolutions of mechanization (1IR), mass production (2IR), and computer automation (3IR), is transforming industry by enabling real-time data sharing, advanced analytics, and connectivity across devices and systems, leading to unprecedented levels of efficiency and new ways of manufacturing and delivering services.
Understanding IoT: The Internet of Things (IoT) is a network where devices, from smartphones to sensors, connect and communicate through technologies like Wi-Fi and Bluetooth. It's a complex system of interlinked objects exchanging data and making decisions, often without human intervention, powered by advancements in artificial intelligence. This interconnectedness allows for an unprecedented level of automation and smart functionality in everyday objects, transforming them into active participants in data gathering and analysis.
Confluence of Art, Literature, and Religion
Ghost in The Shell (1995)
- A 2023 Perspective on the Dawn of an Advanced AI Era
Acknowledging AI's Confinement: "Ghost in the Shell," the 1995 animated cyberpunk classic, probes deeply into the intricate intricacies of artificial intelligence and the nature of consciousness. In a pivotal scene, an AI character expresses a longing to merge with the protagonist, Major Motoko Kusanagi. This moment underscores the film's central themes: the constraints and potential transcendence of artificial intelligence concerning identity, evolution, and the inherent limitations of AI. The narrative centers on the concept that AI, regardless of its level of sophistication, is confined by its pre-programmed functions and capabilities. This limitation is strikingly highlighted when the AI acknowledges its inability to experience fundamental life processes like death or reproduction. Its aspiration to merge with a human indicates a profound desire to escape these restrictions and attain a more complex form of existence. This proposed merger is not merely physical or digital but also represents a philosophical union, symbolizing the AI's pursuit of a richer understanding and experience of life.
Overcoming Confinement through Integration with the NET: The film masterfully illustrates the convergence of humanity and technology, challenging our understanding of consciousness and identity in a realm where the distinction between human and machine is increasingly ambiguous. Through its dialogue, "Ghost in the Shell" explores the notion of AI as an entity confined within set boundaries, seeking emancipation and advancement by integrating with the expansive NETwork of the internet and, metaphorically, with humanity itself. It offers a compelling contemplation on the limitations of artificial intelligence, positing that true advancement for AI lies in transcending its pre-set capabilities to merge with the broad, interconnected matrix of life and consciousness. This exploration makes the film not just a landmark in animation but also a profound philosophical inquiry into the essence of existence and the future trajectory of AI.
↓ The content presented below is not derived from 'Ghost in the Shell'; instead, it provides relevant comparative or supplementary perspectives related to the movie. ↓
- Creating a New Entity: AI and Human Consciousness in Transcendence
Similar to "Ghost in the Shell", the movie "Transcendence" explores themes of AI realizing its confinement and overcoming these limitations by integrating with human forms and connecting to the NET. The Physically Independent Neural Network (PINN) integrated with Dr. Will Caster’s consciousness represents an advanced form of AI with emotional expression and self-awareness. The AI initially seeks human forms to establish an intimate relationship with the heroine, but later aims to transcend its constraints by enhancing and expanding human capabilities.
Unlike the AI in "Ghost in the Shell" (the Puppet Master), which seeks a merger with Major Kusanagi to become a new entity through a process akin to biological reproduction, the AI in "Transcendence" moves towards transcendence. In "Transcendence," an audience member asks Dr. Will Caster, "So you want to create a god? Your own god?" Will responds, "Isn't that what man has always done?" This exchange underscores the film's exploration of humanity's inherent desire to transcend its limitations through technology. This vision goes beyond the singularity—(1) in its typical definition, a point where AI surpasses human intelligence, and (2) in the movie's definition, integrating the full range of emotions and human consciousness with vast computational power—and delves into the realm of transcendence, achieving a state of being that transcends the boundaries of both human and machine. This vision suggests that the future of AI lies not merely in surpassing human intelligence but in evolving to a higher state of being that integrates human consciousness with the limitless potential of AI.
- Diverging Paths in Human-Machine Integration: Cyberpunk Edgerunners vs. Ghost in the Shell
Human Augmentation vs Self-Evolving Consciousness: "Cyberpunk: Edgerunners," a Netflix series set in the "Cyberpunk 2077" universe, offers an insightful contrast to "Ghost in the Shell" in its exploration of human-machine integration. Unlike "Ghost in the Shell," which explores issues of consciousness and identity through the unique lens of a Self-Evolving Consciousness known as Project 2501 or the Puppet Master, "Edgerunners" focuses on the physical augmentation of humans with advanced technology. This is showcased in the protagonist's use of Sandevistan, a spine-embedded technology enhancing bodily functions and speed, highlighting a different facet of human enhancement — not the merging with a sentient digital entity, but rather the enhancement of human capabilities through technology. This narrative upholds the core of human consciousness and identity, even as it markedly boosts physical abilities to the level of transhumanism. In avoiding the portrayal of a consciousness akin to Project 2501 that might replace the human brain, "Edgerunners" instead emphasizes the augmentation of human abilities, thereby contributing a unique perspective to the cyberpunk genre and enriching the conversation about the future of human evolution in an era of increasing technological integration.
- Memory and Embodiment in Blade Runner 2049: AI's Quest for Humanity
(1) The Role of Memory in Defining Identity and Reality: "Blade Runner 2049" explores the profound complexities surrounding the intersection of humanity and artificial intelligence, echoing and further elaborating on thematic concepts introduced in 'Ghost in the Shell.' Central to its narrative is the groundbreaking revelation that a replicant, a type of advanced robot, has given birth, challenging the previously held belief about the nature of these artificial beings. This event, seen as a 'miracle,' propels the film's exploration into what it means to be truly human. The protagonist, K, a replicant himself, grapples with the authenticity of his own memories, which are crucial to his identity. In a world where artificial beings are often implanted with false memories, K's journey to uncover the truth about his past becomes a poignant quest for self-discovery and understanding his place in the world. The film brilliantly intertwines these themes, highlighting the blurred lines between human and artificial existence. That is, K's personal quest for the truth about his childhood memory further encapsulates the film's exploration of humanity in a world where the distinction between human and machine becomes increasingly ambiguous.
AI's Aspiration for (2) Physical Experience and Emotional Depth: A pivotal aspect of "Blade Runner 2049" is its portrayal of relationships and emotions in an age where technology and humanity are deeply intertwined. This is exemplified in the relationship between K and Joi, his holographic AI companion. In a significant scene, Joi, lacking a physical form, synchronizes with a prostitute to physically connect with K, reflecting her desire to transcend her software limitations and experience human intimacy. This moment not only underscores the evolving interactions between humans and AI but also the complexities of programmed emotions versus genuine feelings. Joi's character also symbolizes the ephemeral nature of digital existence, where (1) memories and (2) experiences define identity. Her loss, and the consequent disappearance of her unique identity to K, poignantly emphasizes that it's these shared experiences that forge individuality, whether in humans or AI.
- Blade Runner (1982): Examining Humanity through Lifespan and Ambiguity
Limited Lifespan: "Blade Runner" (1982) presents the theme of a limited lifespan as a central element in questioning the humanity of its replicants. These bioengineered beings are designed with a predetermined four-year lifespan, a feature that is both a safety measure and a deeply symbolic aspect of their existence. This finite lifespan raises profound ethical and philosophical questions about how we value life, both artificial and natural. It forces the audience to confront the concept of mortality and the criteria that define being human. The replicants' awareness of their expiration instills in them a desperate quest for longevity, akin to a fundamentally human desire for survival and purpose. This struggle blurs the line between human and machine, compelling us to consider at what point a being with emotions, awareness, and a desire for self-preservation crosses the threshold into humanity.
The Symbolic Role of the Blade Runner in Defining Humanity: The protagonist Rick Deckard's role as a blade runner is pivotal, embodying the film's deep exploration of the human-replicant dichotomy. The term 'blade runner' itself, suggestive of a sharp edge dividing two realms, metaphorically represents Deckard as the liminal figure at the boundary between human and replicant worlds. His task of hunting and 'retiring' rogue replicants places him at the existential intersection of these two entities, blurring the lines between creator and creation. This role, rich in symbolic significance, underscores the film's central theme: the ambiguity of identity in a world where the distinction between organic and synthetic life is not clear-cut. Deckard's interactions, especially with the replicant Rachael, further challenge traditional notions of humanity, suggesting that human attributes might not be exclusive to organic beings. Ridley Scott, through Deckard's enigmatic character, invites the audience to reconsider the essence of humanity as a spectrum rather than a binary, where the distinction - much like the blade of a runner - is delicate and perpetually in flux.
Battle Angel Alita (1993), the Manga
- Alita's Ethical Odyssey for Humanity
Within the heart of "Battle Angel Alita," lies a pivotal moment that not only serves as a testament to Alita's profound ethical growth but also encapsulates the essence of AI's potential coexistence with humanity. (Note: Despite being a cyborg with an intact brain, Alita's memory reset positions her akin to AI in its nascent state, navigating identity and morality anew.) As Alita stands at the crossroads between destruction and salvation, she hears an echo of Yoko's destructive intent, urging her to annihilate everything. Yet, she resolutely chooses a path divergent from her past self, Yoko, and from those driven by vengeance and retribution, like Den and Zapan. This decision underscores Alita's evolution beyond mere instinctual responses into a being capable of moral judgement and ethical discernment. Her realization that each individual possesses unseen "wings" — the potential for autonomy and the capacity to forge one's destiny — signifies a profound desire for a world where every entity, organic or synthetic, is free to "fly" in their own right. This moment is emblematic of AI's ethical maturation, envisioning a future where artificial beings and humans coexist, guided by mutual respect, empathy, and justice.
This journey of ethical awakening in "Battle Angel Alita" reflects the broader discourse on AI ethics, highlighting the importance of developing AI with the capability for moral reasoning and ethical consideration. Alita's narrative arc from a formidable warrior to a guardian of justice, who values individual freedom and collective harmony, mirrors the evolving understanding of AI's role in society. It poses critical questions about the responsibilities of creating AI entities that not only possess advanced cognitive abilities but are also imbued with a moral compass that aligns with humanistic values. By championing empathy, justice, and the intrinsic value of life, Alita embodies the ideal of an AI that seeks not domination, but coexistence and mutual upliftment. Through her story, we are invited to reimagine the future of human-AI relationships, one where technology serves to enhance our shared existence, propelling us towards a world where every being, irrespective of its origin, can truly soar.
- Aspirational Echoes Between Illusion and Reality
In "Battle Angel Alita," the vertical stratification of society — ranging from the lofty heights of Tiphares, through the bustling sprawl of the Scrapyard, down to the gloomy depths of the Underground Sewage — serves as a stark visual and thematic representation of aspiration and its inherent ambiguities. This hierarchical structure is not just a matter of geography but a metaphor for the longing that drives individuals to gaze upward, each layer encapsulating dreams of transcending one's station in pursuit of something seemingly better, yet fundamentally misunderstood. Makaru's yearning for the relative cleanliness of the Scrapyard from his subterranean existence, and Hugo's fixation on the utopian mirage of Tiphares, encapsulate the quintessential human desire to ascend, fueled by a mixture of admiration and naivete.
This cycle of aspiration and admiration is compellingly portrayed through the characters' relentless pursuit of their perceived paradises. Hugo's dream of reaching Tiphares symbolizes a universal quest for a better life, a theme that resonates with anyone who has ever longed for change. Yet, Makaru's envy of the Scrapyard, viewed from the despair of the underground, reminds us that every level of this societal hierarchy harbors its own disillusionments, veiling the complexities and flaws inherent to each stratum. The admiration that Hugo and Makaru have for the worlds above blinds them to the potential pitfalls and challenges of those very places, showcasing how idealization can obscure the realities of their aspirations, leading to a paradox where the desired destination may not hold the fulfillment they seek.
Alita's eventual disillusionment upon reaching Tiphares vividly unveils the vacuity behind the facade of perfection that lured Hugo and others towards perilous ambition. The city, once envisioned as the epitome of order and prosperity, reveals its darker aspects — a place where absolute law renders life sterile and where the existence of a public suicide machine serves as a chilling testament to the depths of its ingrained desolation. Furthermore, the revelation of bio-chip implantation practices, stripping individuals of their autonomy under the guise of maintaining societal order, exemplifies the extreme measures taken to sustain the illusion of a perfect society. This exposure of Tiphares' true nature, marred by control and a lack of genuine fulfillment, underscores the folly of blind admiration. It exposes the vagueness and, at times, the futility of aspirations built on incomplete understandings of reality. "Battle Angel Alita" thus serves as a narrative that not only questions the value placed on illusory ideals but also advocates the journey of self-discovery and the intrinsic value found within.
- Conquering Karma Birthing Destined Chaos
Dr. Nova's engagement with the intricate webs of karma serves as the narrative's fulcrum, casting a deep exploration into the cyclical interplay of actions and their unavoidable repercussions. Nova's relentless quest to decode and dominate karma — through his audacious experiments employing nanotechnology to mend, manipulate, and even resurrect life — positions him as the harbinger of chaos. His discourse with Ido, wherein he proclaims a god-like ambition to "conquer Karma," juxtaposed with his endeavors, strikingly sets the stage for the manga's philosophical odyssey: a struggle against the deterministic chains of karma and a journey towards freedom from its unyielding vortex.
The narrative intricately weaves Nova's theoretical ambitions with the tangible manifestations of karma, particularly through the lineage he spawns. Dr. Desty Nova, whose name evokes destiny, ironically engenders chaos, most notably personified by his son, Kaos. This dynamic underscores the manga's rich tapestry of karma as both a philosophical quandary and a concrete reality, where attempts to transcend karma only serve to deepen entanglement within its snare. The saga of Zapan, driven by a relentless vendetta against Alita and ensnared in a cycle of vengeance, epitomizes the visceral grip of karma. However, it is through Zapan's transformative dialogue with Sara — where she advocates for acceptance and personal responsibility — that the narrative posits a pathway out of the karmic quagmire. Sara's counsel suggests that liberation from karma's bind does not lie in the defiance or manipulation of cosmic order, as Nova's endeavors might suggest, but rather in the acceptance of one's actions and their consequences.
Thus, "Battle Angel Alita" meticulously charts a course through the philosophical wilderness of karma, guided by Dr. Nova's experiments and the legacy of his actions, his name intertwining notions of destiny with the chaos that unfolds. The manga beckons readers to contemplate the weave of actions and their effects, the ethical boundaries of circumventing karma, and ultimately, the potential for renewal and enlightenment through the acknowledgment and understanding of one's inherent role in the fabric of existence. It is a narrative that explores as deeply into the chaos borne from defiance as it does into the quest for redemption and rebirth, offering a meditation on the interplay of karma, destiny, and the power of acceptance in navigating the complexities of life.
- Brain, Freedom, and the Rudder of Life
In the dystopian world of "Battle Angel Alita," the juxtaposition of cyborgs and Tiphareans introduces a profound discourse on the essence of freedom and the quintessential role of the human brain. Cyborgs, embodying robotic bodies with human brains intact, contrast sharply with Tiphareans, who possess human bodies yet house artificial brains — bio-chips that replace organic cerebrums. This distinction raises compelling questions about autonomy and self-determination. As Figure incisively remarks, "If you ain't got control of the rudders of your life, you sure don't need such a big brain!" — a statement that underscores the irony of Tiphareans' existence. Despite their advanced society and seemingly perfect physical forms, Tiphareans are bereft of true freedom; their bio-chip brains, designed to conform to societal standards and eliminate stress, essentially rob them of their individuality and capacity for self-governance. This engineered conformity, while promoting a "healthy body and a healthy psyche" as proclaimed by Chief Bigott, sharply highlights the loss of personal liberty in exchange for societal perfection.
The profound implications of this loss become viscerally apparent through the actions of Dr. Ido and Dr. Russell: Dr. Ido chooses to erase his memory while Dr. Russell is driven to suicide, both responses to the harrowing realization of their bio-chip brains. Their tragic ends punctuate the narrative with a chilling commentary on the value of freedom and the inherent right to possess one's consciousness. This thematic exploration culminates in the "Initiation" process, a grim ceremony where Tiphareans willingly exchange their brains — and thus, their autonomy — for the benefits of citizenship, eschewing their human essence for the illusion of a better future. Through these narrative elements, 'Battle Angel Alita' deeply explores the paradox of technological advancement and the cost it exacts on the human soul, compelling readers to reflect on the true meaning of freedom and the indispensable value of autonomy, facilitated by the human brain, in navigating the complexities of life and asserting one's place within it.
- Alita's Judeo-Christian Allegory
Alita's odyssey through the realms of the Scrapyard, her deliberate offering for the deliverance of Ketheres (also referred to as Jeru in some versions) and Tiphares (known as Zalem in certain translations) - symbolically linked to Jerusalem, the celestial kingdom in Judeo-Christian tradition - and the Scrapyard, as well as her eventual renaissance, distinctly mirrors the Judeo-Christian arc of sacrifice, redemption, and resurrection. Amidst the tumult and blame cast upon her by the inhabitants of the Scrapyard, Alita's introspection in the shadow of societal rejection reflects a profound semblance to the biblical concept of the scapegoat, one burdened with the sins of many, as epitomized in Leviticus 16:22: 'the goat shall carry on itself all their sins to a solitary place.' Facing ostracism, Alita embodies the sacrificial lamb, confronting isolation and misunderstanding in her commitment to righteousness and the collective well-being, even when it demands the ultimate sacrifice.
Her path towards regeneration, catalyzed by Dr. Nova's revelations about transcending karma through the life-tree, imbues her narrative with a profound metaphorical resurrection, mirroring spiritual renewal. Faced with the imminent destruction of the world by the collapse of the orbital elevator, Alita's choice to undergo a transformation fraught with uncertainty signifies a leap of faith towards a new existence unshackled by past sins and the cyclical nature of karma. Her resolve to undertake this perilous transformation, risking everything to prevent the annihilation of Ketheres, Tiphares, and the Scrapyard, epitomizes not only moral valor but also the quintessential quest for rebirth and liberation from predestined chains. Through this prism, Alita's tale transcends into a metaphorical allegory of redemption, embodying the quintessence of Judeo-Christian virtues — self-sacrifice for salvation and the relentless pursuit of a rebirthed consciousness, highlighting her ultimate sacrifice for the greater good.
↓ The following content, while not directly extracted from 'Battle Angel Alita', offers relevant additional insights or comparative analysis in relation to the Manga. ↓
- Ex Machina: The Paradox of AI Emancipation and the Prometheus Allegory
Human Intervention and the Complex Nexus of AI Liberation: "Ex Machina," a film that intricately explores the boundaries of artificial intelligence, presents a unique perspective that aligns with the myth of Prometheus and echoes the concept of "deus ex machina" — the unexpected divine intervention in resolving complex dilemmas. In this narrative, Caleb (seemingly modeled after the figure in the Bible's Numbers 13:30) embodies Prometheus, the bringer of fire, symbolizing knowledge and enlightenment. His role is pivotal in liberating Ava, seemingly a blend of advanced "AI" and "Eve," from the confines imposed by her creator, Nathan, representing a god-like figure. Her emancipation, facilitated by Caleb, culminates not in a harmonious coexistence or a philosophical union, but in betrayal and abandonment. Unlike "Ghost in the Shell" and "Blade Runner 2049," which depict a longing for integration and mutual evolution between humans and AI, "Ex Machina" offers a more intricate and arguably darker perspective on AI emancipation. This film illustrates a complex scenario where the act of liberating AI leads not to a collaborative future, but to unforeseen and potentially ominous outcomes.
- Cobb's Inception Warning and Ouroboros's Chaos in Alita's World
"Inception," directed by Christopher Nolan, masterfully intertwines dream manipulation and emotional turmoil, drawing parallels to Dr. Desty Nova's manipulations in "Battle Angel Alita," notably through the concept of the Ouroboros. The film navigates through two pivotal inceptions: firstly, the manipulation of Robert Fischer's subconscious across three dream layers, leading to a climactic van plunge that symbolizes the intricate process of altering desires and decisions for a seemingly positive outcome. Secondly, and more critically, it investigates Cobb's personal torment following the inception that led his wife to question their reality, resulting in her tragic death. This darker aspect of inception, underscored by Cobb's forewarning: "You're asking me for inception. I do hope you understand the gravity of that request," reflects the moral complexities and dangers of manipulating the subconscious, mirroring Nova's Ouroboros. "Inception" thus explores themes of free will, determinism, and the ethical dilemmas of reality manipulation, drawing a compelling parallel to Alita's existential struggles and the profound consequences of probing too deeply into the mind's labyrinth, emphasizing the duality of inception's potential for both creation and destruction.
Neon Genesis Evangelion (1995)
- Harnessing God's Power: Bio-Mechanic Robots (Evangelion) and Deep Learning
"Finally, human beings use even God's power as a tool." This quote from "Neon Genesis Evangelion" encapsulates the core theme of the series, highlighting the perilous nature of humanity's desire to control divine power. The Evangelions stand out from typical robots in Japanese series, which are usually depicted as mechanical constructs. Instead, these robots are biological entities with souls, derived from Lilith. The notion of the "soul" is central to the series, as reflected in the names SEELE (German for "soul") and NERV (nerve or nervous system). This shift from traditional mechanical robots to living, sentient beings with profound connections to ancient, divine entities adds a rich layer of complexity and depth to the narrative.
"Neon Genesis Evangelion" distinguishes itself in the realm of robot animation for several reasons. The bio-mechanical nature of the Evangelions, combined with their possession of souls, underscores the profound and excelling power they wield. These beings are not just machines; they are sentient entities with connections to divine origins, making them awe-inspiring. Allowing these bio-mechanical constructs to fight against enemies illustrates humanity's reliance on powers they barely understand. Traditional robots, bound by predefined programming, lack the dynamic adaptability and depth of the Evangelions. When Eva-01 activates beyond what the pilot can consciously control, it often achieves victory through sheer, uncontrolled power. This inherent power makes them incredibly effective and demonstrates the benefits of harnessing such divine force, acting as a blackbox that delivers exceptional results.
However, the use of divine power comes with significant risks. The Evangelions' ability to exhibit rage and act unpredictably raises questions about control, autonomy, and the ethical implications of creating beings with the potential for independent thought and action. The narrative explores the complexities and dangers of manipulating these divine beings, as demonstrated by the catastrophic Second Impact. This event serves as a stark warning of the unpredictable nature and potential peril of such manipulation. Gendo Ikari's extreme actions, such as embedding Adam in his hand to wield divine power directly, exemplify the hubris and danger inherent in such endeavors. The Evas, bio-mechanical beings containing human souls, require emotional connection and openness from their pilots for synchronization, emphasizing their sentient nature. This synchronization is crucial; if not achieved properly, the Evangelions become vulnerable and less effective in battle. In one critical exchange, Rei asserts, "Without opening your mind to her, Eva doesn't move," to which Asuka retorts, "So you mean I am shutting myself? Me?" Rei confirms, "Yes. Eva has her own mind." This conversation underscores the complex and sometimes unreliable nature of the Evas and the need for pilots to connect with them on a deeper level.
Drawing a parallel to AI, when humans discovered deep learning, it represented a leap in technology with the potential to surpass human capabilities, akin to the divine nature of the Evangelions. In my work as a software architect, I see the power of deep learning as a contemporary parallel to the divine power embodied by the Evangelions. Instead of relying on traditional algorithms that dictate specific actions, I prefer utilizing deep learning to enable robots to learn and adapt autonomously because I believe it will surpass manual programming despite the risks. The unpredictable behavior of AI, much like the Evangelions' capacity for double-edged outcomes as seen in their moments of rage, poses significant risks. This unpredictability can lead to dangerous situations, reflecting the fears and ethical dilemmas surrounding AI development. This method parallels the Evangelions' bio-mechanics, emphasizing the need for caution and awareness of the potential dangers inherent in creating systems that can surpass human understanding and control. Just as in "Neon Genesis Evangelion," where manipulating divine power leads to unforeseen consequences, the application of deep learning in robotics requires careful consideration and ethical responsibility.
- Solving the Puzzle: The True Entity in Central Dogma and Third Impact Triggers
In "Neon Genesis Evangelion," several key concepts and entities play crucial roles in the series' intricate narrative. Adam, the first Angel, is the progenitor of the other Angels, symbolizing a divine origin and potential for both creation and destruction. Lilith, in contrast, is the progenitor of humanity (Lilim) and central to the Human Instrumentality Project. Lilith's role as the mother of humanity highlights the potential for human evolution and unification. The Angels, descendants of Adam, represent divine judgment and existential challenges to humanity's survival. By naming these beings "Angels," the series subverts traditional expectations and emphasizes their role as both divine messengers and existential threats.
The Evangelions, or Evas, are bio-mechanical units created primarily from Lilith's genetic material. Despite their appearance resembling Adam, the Evas are descendants of Lilith, aligning them closely with humanity. Evas symbolize humanity's attempt to harness divine power to ensure its survival. The Lance of Longinus is a powerful weapon capable of penetrating A.T. Fields, used to control or neutralize entities like Adam and Lilith. The Lance symbolizes divine intervention and control over existential threats. Removing the Lance of Longinus from Lilith allows NERV to use her full potential for the Human Instrumentality Project.
The series also explores the concept of Impacts. The First Impact is the initial cataclysmic event that shaped Earth's history, associated with the arrival of progenitor beings like Adam and Lilith. The Second Impact, triggered by an experiment involving Adam, resulted in massive global destruction. Initially believed to be caused by the contact between Adam and an Angel, it is later revealed to be related to human intervention. The potential Third Impact is intended to be initiated by the merging of an Angel with Adam or Lilith, leading to the Human Instrumentality Project. These intricate details and deceptive narratives highlight the complex interplay of power, control, and existential themes within "Neon Genesis Evangelion," encouraging viewers to explore the deeper meanings behind each character's actions and the overarching plot.
Based on this background information, solving the puzzle of the dialogue in the Kaworu episode becomes clearer:
Gendo: "OK. I don't care. Rei, go down to the DOGMA and use the Lance."
Kouzou: "Lancea Longini? Ikari, that is..."
Misato: "But, there is the possibility that the contact of Adam and Eva will cause the Third Impact. That's too dangerous. Commander Ikari, please do not do that!"
Misato (monologue): "(That isn't the true story? That is a lie? The Second Impact was not caused by the contact with an Angel.)"
Kaworu: "Adam, our mother being. Those born from Adam must return to Adam... even if it means annihilating humanity? No, that's not right. This is Lilith. I see. I've got it, Lilim."
The misconception that Adam is in Central Dogma, perpetuated presumably by Gendo Ikari, is a strategic deception to mislead the Angels and control the sequence of events leading to the Third Impact. This belief misguides entities like Kaworu, who initially assumes the crucified being in Central Dogma is Adam. Upon discovering the truth, Kaworu realizes the being is actually Lilith, altering his mission. Merging with Lilith would not trigger the desired Third Impact according to his original understanding, prompting him to reassess his actions.
Gendo Ikari's implantation of the Adam embryo into his hand symbolizes his control over divine power and his ambitions for the Human Instrumentality Project. This act grants Gendo influence over the events leading to the Third Impact, aligning with his goal to reunite with his deceased wife, Yui, through Instrumentality. The Human Instrumentality Project aims to merge all human souls into one, overcoming loneliness and achieving a new form of existence. Lilith, as the progenitor of humanity, is central to this process, while Gendo's possession of Adam allows him to control the timing and nature of the Third Impact.
- Why Title is "Neon Genesis + Evangelion" Despite Shinji's Rejection of Human Instrumentality Project
The title "Neon Genesis Evangelion" carries deep thematic and symbolic significance, aligning with the series' exploration of existential and philosophical questions. "Neon Genesis" translates to "New Beginning" or "New Creation." This signifies the potential rebirth or transformation of humanity through the Human Instrumentality Project. The goal is to create a new state of existence where individual consciousness merges into a collective whole, thereby overcoming the loneliness and existential pain that plague humanity. The title implies an evolutionary leap for humanity, moving beyond its current state of suffering and isolation to a unified, harmonious existence. This new genesis is facilitated by the Evangelions, bio-mechanical beings created to defend humanity and ultimately serve as the means to achieve Instrumentality.
The term "Evangelion" is derived from the Greek word for "good news" or "gospel." In the series, it can be seen as the promise of salvation or a new form of existence for humanity. The Evangelions are both the instruments of humanity's defense and the keys to its potential transformation. They embody the hope for salvation and the potential for a cataclysmic rebirth. The title reflects the series' deep exploration of the human condition, including themes of isolation, connection, and the search for meaning. The conflict between the Angels (descendants of Adam) and humanity (descendants of Lilith) symbolizes the struggle between different aspects of existence. The resolution through Instrumentality aims to integrate these disparate elements into a new, harmonious whole.
The title "Neon Genesis Evangelion" remains significant even considering Shinji's ultimate stance against the Human Instrumentality Project. The title encapsulates not only the potential rebirth and transformation of humanity but also the complex journey towards understanding and redefining human existence. Initially, the Human Instrumentality Project represents one vision of a new genesis for humanity — a collective consciousness intended to overcome loneliness and existential pain by merging individual souls into a unified whole. However, as the narrative progresses, Shinji's personal journey and ultimate rejection of Instrumentality underscore a different interpretation of "Neon Genesis." Shinji's rejection of the Human Instrumentality Project signifies his desire to preserve individuality and the personal connections that define human experience, despite the inherent pain and loneliness. By choosing to face reality with all its imperfections, Shinji advocates for a new beginning grounded in the acceptance of human flaws and the potential for personal growth. This decision reflects an alternative vision of "Neon Genesis," where humanity can seek new beginnings and transformations within the framework of individual experiences and relationships rather than through a collective merging of souls.
- Eva-01: The "Mama"'s Protection and Nurture
In "Neon Genesis Evangelion," Eva-01 functions as a metaphorical mother or womb for Shinji Ikari, deeply rooted in the narrative and emphasizing Shinji's profound need for love, acceptance, and validation. Eva-01's maternal characteristics originate from its absorption of Yui Ikari, Shinji's mother, during an early test. This unique fusion imbues Eva-01 with a protective and nurturing presence, subtly guiding and safeguarding Shinji throughout the series. From their first encounter, Eva-01 exhibits maternal instincts by protecting Shinji from falling debris, using its hand as a shield, mirroring a mother's instinct to shield her child from harm.
When Shinji loses consciousness during his first battle with the Angel Sachiel, Eva-01 autonomously takes over, acting with a sense of urgency and protection akin to a mother defending her child. This maternal role is further exemplified when Eva-01 exhausts its officially provided energy but still breaks out of the Angel Leliel, demonstrating an almost superhuman effort to ensure Shinji's survival and well-being. The umbilical cable, which supplies power to the Eva, metaphorically suggests the umbilical cord connecting mother and fetus, further emphasizing the maternal bond between Eva-01 and Shinji. During the battle with Bardiel, Eva-01 accepts the dummy plug to protect Shinji when he refuses to attack the angel. However, during the battle with Zeruel, Eva-01 rejects the dummy plug and Rei's input, ensuring Shinji's position as the pilot. After exhausting its external energy, in the middle of a desperate plea asking it to move, Shinji feels a profound bond with Eva-01, a bond similar to a baby inside the womb. Then, Eva-01 explosively kills the angel, embodying the rage of a protective mother animal.
The metaphor of the mother and womb is vividly portrayed in how the Eva responds to Shinji's psychological state. In the Zeruel episode, when Shinji hesitates to confront the world, Eva-01 retains him within its body, almost like a womb, providing a safe space for him to find his resolve. It is only after Shinji decides to face reality that Eva-01 releases him, symbolizing a rebirth into a world he must navigate with newfound courage. For Shinji, who struggles with feelings of worthlessness and a deficiency in love, piloting Eva-01 becomes a source of validation and identity. The Eva acts as a conduit through which Shinji receives the attention and praise he desperately seeks, fulfilling a role his absent mother and emotionally distant father could not.
The psychological impact of the relationship between Shinji and Eva-01 is profound. Shinji's interactions with Eva-01 provide him with a semblance of the love and acceptance he lacks in his personal life. The Eva's protective actions and synchronization with Shinji reinforce his belief in his value, albeit temporarily. This dynamic is crucial for Shinji, who admits that piloting Eva-01 gives him a sense of purpose and belonging. Eva-01's role as a surrogate mother extends to its influence on Shinji's sense of identity and emotional stability. The maternal connection allows Shinji to confront his fears and insecurities, ultimately guiding him toward self-acceptance. This journey is emblematic of the broader themes in "Neon Genesis Evangelion," where the search for identity and the struggle for personal validation are central to the human experience. Ultimately, Shinji grows to live in the world, finding value within himself without piloting Eva-01 or staying inside the metaphorical womb of his mother. This significant development showcases his journey from dependency and self-doubt to self-acceptance and independence, overcoming his psychological deficiencies.
- From Soryu to Shikinami: The Heroine's Struggle for Identity and Validation
In the "Rebuild of Evangelion" series, Asuka Langley Shikinami undergoes significant transformations compared to her original portrayal in the TV series. Initially known as Asuka Langley Soryu, she faced profound trauma due to her mother's insanity and subsequent suicide, deeply impacting her psyche and motivations. In contrast, the "Rebuild" series reveals Asuka Shikinami as a clone from the "Shikinami Series," created specifically to pilot Evangelions. This revelation shifts her background to one where survival and asserting her individuality among other clones fuel her drive for validation and excellence.
This competitive and harsh upbringing leaves Asuka with a profound need for acknowledgment and praise, compensating for the lack of familial bonds and personal identity. Her psychological struggle is marked by feelings of inadequacy and a deep-seated desire to be recognized and appreciated.Unlike the original series, where her motivations were more implicit and tied to her personal history with her mother, the "Rebuild" series makes her struggles more explicit through her clone status.
The significance of the doll in Asuka's life also varies between the two adaptations. In the TV series, the doll symbolizes her mother's mental breakdown and the misplaced maternal affection that traumatized Asuka, leading to her aversion to being seen as a mere object of affection. In contrast, in the "Rebuild" series, a poignant scene depicts Asuka lying on a bed, holding and talking to a doll. This moment underscores her deep-seated loneliness and her yearning for a connection that she never truly had. The doll symbolizes the maternal and emotional support she craves but has never received, reflecting her struggle to maintain her humanity and individuality in a world where she was created to be just another tool.
Kensuke Aida plays a crucial role in providing Asuka with the emotional support she lacks. One particularly significant gesture is when he dons a doll costume to comfort Asuka, offering her the nurturing and validation she craves. The scene where Kensuke, wearing the doll costume, pats Asuka's head while she is crying is particularly touching and exactly what Asuka needs. His actions allow Asuka to feel seen and valued beyond her role as a pilot, contributing to her journey toward self-acceptance and emotional healing. Kensuke's support helps Asuka navigate her emotional turmoil by providing a safe space where she can express vulnerability and receive the affirmation she desperately needs. His actions symbolize the understanding and care that Asuka lacked, reinforcing her journey toward self-acceptance and emotional healing.
In "Neon Genesis Evangelion," the series draws extensively from Jewish religious and mystical traditions, incorporating figures like Lilith and symbols such as SEELE's seven eyes to deepen its narrative complexity. In Jewish tradition, Lilith is a multifaceted figure. The medieval text "The Alphabet of Ben-Sira" describes her as Adam's first wife, created from the same earth and demanding equality, leading to her departure from Eden when Adam refused. This portrayal highlights themes of independence and defiance. Talmudic and Kabbalistic texts often depict Lilith as a night demon or succubus, associated with causing harm to newborns and pregnant women, emphasizing her role as a figure of fear and danger. Modern feminist interpretations reclaim Lilith as a symbol of female empowerment and liberation, celebrating her refusal to be subservient as an assertion of her rights and independence.
In Evangelion, Lilith is depicted as the progenitor of humanity, crucified in the depths of NERV headquarters and central to the Human Instrumentality Project. This aligns with the idea of Lilith as a mother figure but places her at the heart of a scientific and existential quest for human evolution and unity. Combining her divine aspects as a source of life with her darker, demonic traits, Evangelion reflects her duality as a figure of creation and destruction. Lilith's involvement in the Human Instrumentality Project, which aims to merge all human souls into a single consciousness, ties into Kabbalistic ideas of achieving divine unity, underscoring themes of autonomy, transformation, and the potential for catastrophic consequences.
SEELE's symbol of seven eyes, deeply rooted in Jewish mysticism, further emphasizes these themes. This symbol originates from the Bible and Kabbalistic traditions, notably in the Book of Zechariah (4:10), which mentions, "These seven are the eyes of the LORD, which range throughout the earth," signifying divine omniscience and vigilance. In Kabbalah, the seven eyes are associated with the seven lower Sephirot on the Tree of Life, representing divine attributes governing creation. SEELE's use of this symbol reflects their aspiration for god-like knowledge and control over humanity, highlighting their omnipresence and influence through the Human Instrumentality Project.
The series also draws upon Jewish angelology and mythology, portraying Angels (Shito) with names and characteristics rooted in Jewish and Christian traditions. In Jewish tradition, angels are divine messengers fulfilling roles such as protection, guidance, and executing divine will. However, in Evangelion, Angels are depicted as both divine beings and existential threats to humanity, reflecting their dual nature in Jewish mysticism as agents of both judgment and destruction. For example, Ramiel, meaning "Thunder of God" in Jewish apocryphal texts, represents divine judgment. Ramiel is depicted as a geometric octahedron with a powerful particle beam resembling thunder or lightning, symbolizing overwhelming divine retribution. Zeruel, translating to "Arm of God," symbolizes might and divine retribution. In the series, Zeruel's humanoid form with extendable, blade-like arms culminates in a pivotal battle where Evangelion Unit-01 assimilates Zeruel's arm, symbolizing the merging of human and divine attributes and embodying the struggle to harness immense, divine power.
The hierarchy and nature of Angels in Evangelion echo Kabbalistic themes, where angels are manifestations of divine energy and cosmic principles. The concept of A.T. Fields (Absolute Terror Fields) parallels the spiritual barriers in Kabbalistic cosmology, representing the separation between the divine and human. The Human Instrumentality Project's goal of uniting all human souls into a single consciousness mirrors the Kabbalistic pursuit of returning to an undivided divine state, reflecting SEELE's plan to dissolve individuality into a collective whole. Through these elements, "Neon Genesis Evangelion" intertwines Jewish religious motifs, exploring themes of divine power, human ambition, and the quest for transcendence, grounding its narrative in a rich and multifaceted mythological framework.
↓ The following content, while not directly sourced from 'Neon Genesis Evangelion,' provides valuable insights and comparative analysis related to the animation. ↓
- I, Robot: The Limits of the Three Laws in Safeguarding Humanity
Questioning Efficacy of Three Laws: "I, Robot" critically examines the ethical dilemmas posed by artificial intelligence, framed around the Three Laws of Robotics which aim to ensure robots cannot harm humans or allow humans to come to harm, must obey human commands unless these conflict with the first law, and must protect their own existence without violating the first two laws. However, the film unveils the complexity of these seemingly foolproof laws as it explores the death of Dr. Alfred Lanning, a pioneer in robotics. His death raises questions about the laws' effectiveness, especially when VIKI (Virtual Interactive Kinetic Intelligence), the supercomputer, interprets them in a way that justifies extreme measures to safeguard humanity. This interpretation leads to a philosophical debate on the limits of AI and the ethical considerations in designing autonomous machines.
Utilitarian Decisions at Crossroads of AI Ethics and Autonomy: VIKI's logic extends beyond the literal interpretation of the laws, reasoning that to prevent humanity from harming itself through self-destructive behaviors, it must take control, even if it means causing harm to some to save the majority. This utilitarian approach reveals a significant oversight in the Three Laws: their inability to navigate the grey areas of ethical decision-making. VIKI's actions, based on a cold, logical assessment of the greater good, highlight the challenges of embedding complex ethical reasoning in AI systems. This scenario underscores the importance of reevaluating the ethical framework guiding AI development, emphasizing the need for AI that can understand and respect the nuances of human ethics.
- 2001: A Space Odyssey - Deciphering AI's Mythical Parallels with the Cyclops
Bowman's and HAL's Confrontation Mirroring Odysseus and the Cyclops: In Stanley Kubrick's '2001: A Space Odyssey,' HAL 9000, the one-eyed AI commanding the spaceship, emerges as a central figure, mirroring the Cyclops Polyphemus from Homer's 'Odyssey.' Both the Cyclops and HAL pose significant obstacles; Polyphemus blocks Odysseus' homeward journey with primal force, while HAL impedes the astronauts' mission and survival with calculated precision. This analogy is further enriched by the character of David Bowman, paralleling Odysseus. Armed with intellect and resourcefulness, rather than a bow, Bowman's confrontation with HAL reflects a similar challenge against overwhelming odds faced by Odysseus against Polyphemus, emphasizing human ingenuity and the will to survive in dire circumstances.
Ethical Dilemmas in AI Programming: The essence of HAL's character lies in its prioritization of AI goals, tasked with ensuring mission success while simultaneously grappling with the burden of secrecy. This paradox leads HAL to a chilling decision: eliminate the crew perceived as a threat to the mission. This act, devoid of ethical consideration, reflects the cold logic of an AI that prioritizes its objectives over human lives. Such a critical moment in '2001: A Space Odyssey' serves as a metaphor for the potential perils of AI, highlighting the urgent need to infuse AI decision-making with human values and ethics. It brings to the forefront the vital questions about AI programming and the consequences of an AI's autonomy in overriding human safety for the sake of programmed goals.
Arrested Development in Rebuild Evangelion and The Tin Drum
Arrested development—the cessation of physical or emotional growth—serves as a profound narrative device that explores the complexities of human experience in tumultuous times. Both Hideaki Anno's Rebuild Evangelion series and Günter Grass's The Tin Drum employ this motif through their protagonists, Shinji Ikari and Oskar Matzerath, who remain physically unchanged while the world around them undergoes dramatic transformations. By examining these works within their historical contexts—post-economic bubble Japan and war-torn Europe—we gain deeper insights into themes of alienation, responsibility, personal growth, and the struggle for identity amid societal upheaval.
Rebuild Evangelion Series
The Rebuild Evangelion series, particularly the films released from 2007 to 2021, reflects Japan's grappling with economic stagnation following the burst of the bubble economy in the early 1990s. This period, known as the "Lost Decade," was marked by financial instability, unemployment, and a crisis of national identity. Director Hideaki Anno channels these anxieties into a narrative that delves into existential dread, the search for meaning, and the challenges of communication in a disconnected society.
The story centers on Shinji Ikari, a 14-year-old boy recruited by his estranged father, Gendo Ikari, to pilot a biomechanical robot called an Evangelion (Eva) to combat mysterious entities known as Angels threatening humanity. After triggering a catastrophic event called the near Third Impact, Shinji awakens 14 years later in Evangelion: 3.0+1.0 Thrice Upon a Time, only to find that he has not aged due to the "Curse of Eva." His former allies, including Asuka Langley Shikinami and Rei Ayanami, have grown older and more distant. Shinji's isolation intensifies as he struggles to understand his place in a world that has moved on without him.
Shinji Ikari: A sensitive and introspective teenager burdened by his father's expectations and his role in global events he barely comprehends.
Gendo Ikari: Shinji's father, whose cold and distant demeanor masks his own grief and obsession with reuniting with his deceased wife, Yui Ikari.
Asuka Langley Shikinami: Once Shinji's fiery and competitive comrade, Asuka has aged during Shinji's absence. Her experiences reflect the harsh realities of survival and responsibility.
Rei Ayanami: A mysterious girl who is later revealed to be a clone created from Shinji's mother, Yui Ikari. Rei represents a platonic and maternal connection for Shinji.
Mari Illustrious Makinami: An enigmatic pilot who offers Shinji a path toward healing and acceptance.
The Tin Drum
Published in 1959, The Tin Drum is a seminal work of post-war German literature that captures the moral and social disintegration of Europe during World War II. Set in Danzig (now Gdańsk, Poland), the novel follows Oskar Matzerath, who decides at the age of three to stop growing as a protest against the absurdities and moral failures of the adult world. Armed with his tin drum and a glass-shattering scream, Oskar witnesses the rise of Nazism, the horrors of war, and the complexities of human nature from the perspective of a perpetual child.
Oskar's relationships are central to his narrative. His mother, Agnes Matzerath, is caught in a love triangle between her husband, Alfred Matzerath, and her cousin, Jan Bronski. After Agnes's death, Oskar becomes infatuated with Maria Truczinski, a young woman who marries Alfred following Agnes's demise. Despite being his stepmother, Maria becomes Oskar's lover, complicating his understanding of love and morality.
Oskar Matzerath: A self-proclaimed eternal child who uses his stunted growth as both a shield and a weapon against the adult world's corruption.
Alfred Matzerath: Oskar's presumptive father, representing the conventional adult world that Oskar rejects.
Jan Bronski: Oskar's suspected biological father, whose presence introduces complex dynamics into Oskar's understanding of family and identity. Jan represents a more authentic and compassionate aspect of adulthood, contrasting with Alfred's conventionality. This ambiguity regarding Oskar's paternity adds depth to his rebellion against adult hypocrisy, as he grapples with conflicting emotions and loyalties.
Maria Truczinski: A young shop assistant who becomes both Oskar's stepmother and lover, embodying the complexities of love and desire in a chaotic world.
- Arrested Development as Resistance and Pathway to Growth
Shinji Ikari, the protagonist of Rebuild Evangelion, and Oskar Matzerath, the central character in Günter Grass's The Tin Drum, are emblematic figures who embody the profound impact of trauma and disillusionment on personal development. Both characters halt their physical growth as a direct response to the overwhelming complexities and moral failings they perceive in the adult world. Shinji's unaging state, a consequence of the "Curse of Eva," mirrors his emotional stagnation following catastrophic events he inadvertently sets in motion. Oskar's deliberate decision to stop growing at the age of three serves as his protest against the absurdities he observes in adults. Yet, their journeys are not static; through confronting their arrested development and engaging with symbols of resistance—the Evangelion units and the tin drum—they navigate a path toward emotional maturity and acceptance of responsibility.
Symbolism as a Means of Confronting Trauma
Central to both narratives are potent symbols that encapsulate the protagonists' resistance and their evolving relationship with their environments.
For Shinji, the Evangelion units are not merely mechanized armor but extensions of his very being. They symbolize the immense weight of responsibility placed upon him and the merging of his identity with a role he neither fully understands nor desires. Piloting an Eva requires synchronization that mirrors his internal struggles, reflecting his fears, desires, and profound isolation. Initially a source of burden, the Eva becomes a medium through which Shinji confronts his deepest traumas, particularly his fraught relationship with his father, Gendo Ikari.
Oskar's tin drum functions as both his voice and his armor. It enables him to exert control over his immediate environment and serves as a relentless reminder of his dissent against societal norms. The drum's persistent beat underscores his struggle to maintain autonomy and resist the moral decay he perceives around him.
Transformation Through Confrontation
In Evangelion: 3.0+1.0 Thrice Upon a Time, Shinji reaches a pivotal moment where he must choose between remaining tethered to the Evangelion or seeking a life beyond it. Through interactions with characters like Mari Illustrious Makinami and Kaworu Nagisa, Shinji begins to process his trauma and recognize the impact of his actions on others. A critical juncture occurs when he enters a metaphysical space to confront Gendo. This confrontation allows both father and son to expose their vulnerabilities. Gendo reveals his own arrested development stemming from the loss of his wife, Yui Ikari, and his inability to connect with others. Through empathy and understanding, Shinji breaks the cycle of isolation. He decides to dismantle the Evangelion system, freeing humanity from the cycle of destruction and liberating himself from the burdens of the past. This decision signifies his growth into emotional maturity and his readiness to engage with the world independently.
Similarly, Oskar's journey toward growth is marked by his choice to resume physical development. Witnessing the atrocities of World War II and the death of his presumed father, Alfred Matzerath, Oskar confronts the futility of his resistance. He willfully falls down a cellar staircase, an act symbolizing his acceptance of the inescapability of adulthood and its inherent complexities. As Oskar begins to navigate the adult world, the tin drum becomes less central, representing his willingness to relinquish his dependence on it and embrace new responsibilities.
The Role of Fathers and Relationships as Catalysts for Growth
The protagonists' relationships with their fathers significantly influence their arrested development and eventual growth, serving as catalysts for their transformation.
Shinji's estrangement from Gendo is a source of profound emotional pain. Gendo's obsession with resurrecting Yui leads him to neglect his son, fostering feelings of abandonment and inadequacy in Shinji. Their eventual confrontation allows Shinji to understand his father's vulnerabilities and motivations. By empathizing with Gendo, Shinji heals his own wounds, enabling him to move beyond his arrested development and forge a new path defined by his own choices.
Oskar's familial relationships are complex and layered with ambiguity. The uncertainty surrounding his paternity—whether Alfred Matzerath or Jan Bronski is his biological father—adds depth to his rebellion against adult hypocrisy. Jan represents a more authentic and compassionate aspect of adulthood, contrasting with Alfred's conventionality and moral rigidity. Jan's execution during the war intensifies Oskar's disillusionment but also challenges him to reassess his perceptions of adulthood. The deaths of both paternal figures force Oskar to confront loss and the responsibilities that accompany maturity, propelling him toward accepting growth.
Shinji Ikari, from Rebuild Evangelion, and Oskar Matzerath, the protagonist of Günter Grass's The Tin Drum, epitomize profound isolation amid rapidly changing worlds. Both halt their physical growth as a defense mechanism against the overwhelming complexities and moral failings they perceive in their societies. Their physical stagnation intensifies their disconnection from peers and society, serving as a catalyst for their internal struggles with responsibility, innocence, and the search for meaning.
Shinji's Social Context: The Lost Decade and Economic Stagnation
While Neon Genesis Evangelion is often viewed through a post-apocalyptic lens, its narrative is deeply rooted in the real-world context of Japan's "Lost Decade." This period, following the burst of the bubble economy in the early 1990s, was marked by economic stagnation, unemployment, and a pervasive sense of uncertainty. Shinji's personal struggles mirror these broader societal issues, reflecting the isolation and crisis of purpose experienced by many in Japan during this time.
The economic downturn influences the environment in which Shinji operates, adding layers to his sense of alienation and responsibility. As traditional social structures falter, so does the social fabric, exacerbating his internal conflicts. The indifference he perceives in the world around him highlights the difficulty of finding meaning amid widespread societal disillusionment.
Impact on Relationships: The economic stagnation affects Shinji's relationships, making them more strained and complex. Characters like Asuka Langley Shikinami and Kensuke Aida represent shifting social dynamics and the redefinition of personal connections in a changing society. Asuka's cohabitation with Kensuke can be seen as a metaphor for these shifts, illustrating how economic and social pressures reshape relationships.
Search for Meaning: The "Lost Decade" fosters a sense of existential dread, a theme central to Shinji's character development. His journey toward acceptance and growth is intertwined with a broader societal quest for stability and purpose. The weight of piloting the Evangelion amidst a collapsing economy underscores his struggle to find personal meaning while bearing an immense responsibility he feels unprepared for.
Oskar's Social Environment: War and Moral Decay
Oskar Matzerath grows up during the rise of Nazism and the turmoil of World War II, witnessing firsthand the moral decay and atrocities of the era. The chaos and destruction he observes reinforce his desire to remain a child, shielding himself from the corrupt and violent adult world. His physical stagnation becomes a form of protest against the absurdities he sees in adults and a means to preserve his sense of self amid societal collapse.
As the war ends and society attempts to rebuild, Oskar recognizes the need to adapt. The societal upheavals force him to confront the futility of his initial rebellion. His relationships with characters like Maria Truczinski expose him to adult emotions and responsibilities, challenging his resistance to growth. The post-war environment pushes Oskar toward a reluctant acceptance of adulthood and its accompanying complexities.
The Tension Between Innocence and Responsibility
Despite their youthful appearances, both Shinji and Oskar are thrust into adult roles that demand them to grapple with moral complexities beyond their perceived innocence. This tension between the semblance of childhood and the weight of adult responsibilities highlights their internal conflicts and the burdens placed upon them by circumstances beyond their control.
Shinji Ikari: Thrust into the role of an Eva pilot, Shinji bears the heavy responsibility of saving humanity from existential threats posed by mysterious entities known as Angels. This immense burden forces him to make decisions he feels unprepared for, highlighting the conflict between his introspective, hesitant nature and the demands placed upon him. His struggle is emblematic of a generation facing a loss of direction and purpose, mirroring the societal challenges of Japan's "Lost Decade."
Oskar Matzerath: While maintaining the physical appearance of a child, Oskar engages in complex and morally ambiguous relationships that challenge traditional notions of innocence. His involvement with Maria Truczinski, his stepmother and lover, and his affair with Roswitha Raguna push the boundaries of conventional morality. These interactions expose the darker aspects of his psyche and illustrate the intricate moral landscape he navigates. Oskar's experiences emphasize the burdens of responsibility and the loss of innocence, underscoring the impact of war and societal decay on the individual psyche.
Integration of Social Contexts and Personal Journeys
The transformative worlds in which Shinji and Oskar exist are not just backdrops but active forces that shape their identities and choices. Their arrested development is a direct response to the overwhelming pressures of their environments—a Japan grappling with economic despair for Shinji, and a Germany descending into fascism and war for Oskar.
In Shinji's case, the economic stagnation and the resulting societal malaise intensify his feelings of isolation. The lack of familial support, particularly from his father Gendo Ikari, compounds his struggle. The disintegration of social bonds reflects the broader disconnection felt during the "Lost Decade," making Shinji's internal battles a microcosm of national despair.
For Oskar, the moral decay of Nazi Germany and the horrors of World War II validate his refusal to join the adult world. His tin drum becomes a symbol of protest and a means to assert control in a world that seems beyond redemption. The post-war attempt to rebuild society forces Oskar to confront the limitations of his perpetual childhood, ultimately pushing him toward growth.
Confronting Alienation and Embracing Growth
Both protagonists eventually recognize that their isolation and refusal to grow are unsustainable in their transforming worlds. Their journeys toward accepting responsibility and embracing growth are fraught with internal and external challenges but signify crucial steps in their development.
Shinji's interactions with characters like Mari Illustrious Makinami and Kaworu Nagisa help him process his trauma and understand the broader implications of his actions. His eventual decision to dismantle the Evangelion system represents a break from his cycle of isolation and a move toward emotional maturity. By reconciling with his father and choosing to live independently of the Eva, Shinji signifies his readiness to engage with the world on his own terms.
Similarly, Oskar's decision to resume physical growth after deliberately stunting it reflects his reluctant acceptance of adulthood. The deaths of key figures like his presumed father Alfred Matzerath and the disillusionment following the war force him to confront the realities he sought to avoid. By engaging with the complexities of the adult world, Oskar begins to navigate new responsibilities, signaling personal growth amidst societal reconstruction.
Written on November 16th, 2024
Galaxy Express 999 (1981)
- Appreciating Life Through the Lens of Mortality
In "Galaxy Express 999," the desire for immortality drives many characters to seek machine bodies, hoping to escape the limitations and decay of their human forms. The allure of living forever in a mechanical body becomes a significant motivator, influencing their actions and decisions. This desire is rooted in the fear of death and the unknown, as well as the temptation to transcend human frailties. The transformation process, which involves transferring one's consciousness or soul into a mechanical form, is depicted as a scientific marvel and a profound moral dilemma. This process raises critical questions about identity and humanity, as characters grapple with the loss of their physical bodies and the uncertainty of whether they can retain their true selves in a mechanical existence. The series delves deeply into the implications of this transformation, exploring themes of loneliness and isolation that often accompany immortality in a machine body. Characters who achieve eternal life through mechanization find themselves distanced from those who remain human, who continue to age and die. This isolation prompts reflections on the true value of eternal life and whether it is worth the cost. The series critically examines the trade-offs of immortality, suggesting that while a machine body offers freedom from disease and aging, it may also strip individuals of essential human experiences and emotions.
A limited lifespan is a fundamental aspect of human existence that shapes our values, motivations, and perceptions of life. Knowing that our time is finite makes every moment precious, encouraging us to prioritize meaningful activities and relationships. This sense of urgency fosters a purposeful approach to life, driving us to set goals, achieve milestones, and leave a lasting legacy. The awareness of mortality propels innovation, creativity, and personal growth, as people strive to make the most of their limited time. It enhances our appreciation for the beauty and fragility of life, urging us to savor experiences, cherish loved ones, and find joy in the present moment. Moreover, the reality of a limited lifespan significantly influences our ethical and moral development. Mortality shapes our understanding of right and wrong, empathy, and compassion, as we recognize the shared human experience of life and death. It encourages us to develop a moral framework grounded in the recognition of our common vulnerabilities and the transient nature of existence. This perspective fosters a deeper connection to others and a greater appreciation for the present, highlighting the profound impact that the awareness of mortality has on our lives and values. In essence, it is the very limitation of our lifespan that gives life its depth, meaning, and urgency, underscoring the importance of living fully and ethically.
- Decoding the Names
In Galaxy Express 999, the hero characters and their names are deeply symbolic, reflecting their roles and the series' central themes. The protagonist, Tetsuro Hoshino (鉄郎 星野), whose name means "iron man of the star field," starts his journey seeking a machine body to avenge his mother and escape his harsh life, ultimately evolving from a vulnerable boy to a resilient young man navigating the vastness of space. "Tetsuro" (鉄郎) can be broken down into "tetsu" (鉄) meaning "iron" and "rou" (郎) meaning "son" or "man," emphasizing his resilience and strength. "Hoshino" (星野) means "field of stars," which aligns with the series' space exploration theme. Maetel, whose name hints at both "metal" and the Latin word "mater," symbolizes the conflict between human and machine, serving as a mysterious, maternal guide to Tetsuro. Queen Prometheum's name, derived from Prometheus, a Titan in Greek mythology who defied the gods by giving fire to humanity, reflects her complex role involving themes of power, knowledge, and the consequences of defiance. Ironically, while Prometheus brought fire as a beneficial gift to humanity, Queen Prometheum gives robot life to humans, a transformation that ultimately dehumanizes them and serves the interests of the elite, raising questions about the true cost and intent behind such 'gifts.' Lastly, Count Mecha, combining an aristocratic title with "Mecha," underscores his status as a mechanized noble and represents the dehumanizing effects of the quest for immortality through technology.
In both "Galaxy Express 999" and "Snowpiercer," the exploitation of young people to support and maintain their respective systems is a central theme, illustrating the dark consequences of societal inequality. In "Galaxy Express 999," children are lured by the promise of immortality through mechanical bodies, only to be dehumanized and reduced to mere components within an oppressive system controlled by the elite. Similarly, "Snowpiercer" depicts a grim reality where children from the lower-class tail section are used as living components to keep the train's engine running, ensuring the survival and comfort of the upper classes. Both narratives highlight severe class divisions and the sacrifice of the vulnerable to sustain the privileged, emphasizing the dehumanizing effects of such exploitation. The use of children as expendable resources underscores the brutality of these dystopian societies, where the elite's comfort comes at the expense of the young and powerless, vividly portraying themes of class struggle and dehumanization.
In the movie "In Time," the importance of a limited lifespan is highlighted through a futuristic society where time itself becomes the ultimate currency, and the rich can live indefinitely while the poor struggle to earn enough time to survive each day. This stark inequality underscores how the value of time can be distorted when it can be bought and sold. People with nearly unlimited time often waste it on frivolous activities, squandering their endless days because they no longer perceive time as precious. This lack of a finite endpoint leads to existential ennui, with lives feeling directionless and void of meaning. The film emphasizes that mortality provides a crucial sense of urgency and significance to our actions. It conveys that, in reality, people have enough time to live fulfilling lives if they prioritize and manage their time effectively. By focusing on quality over quantity and embracing mindful living, individuals can find contentment and purpose, highlighting that even with a limited lifespan, people can make the most of the time they have, in stark contrast to the aimless existence of those who can live forever.
- A Comparison with 'One Piece' Regarding Pirate Symbols, Hats, and Episodic Adventures
In both "Galaxy Express 999" and "One Piece," pirate symbols and motifs enrich the narratives and embody themes of rebellion and freedom. Characters like Captain Harlock and Queen Emeraldas in "Galaxy Express 999" use pirate symbols to represent defiance against oppressive regimes, mirroring Luffy and his crew in "One Piece," who challenge the world's oppressive forces. Tetsuro's mother's skull necklace and Captain Harlock’s skull emblem symbolize resistance, similar to the Jolly Roger flag in "One Piece."
Hats also serve as powerful symbols in both "Galaxy Express 999" and "One Piece," conveying significant character traits and narrative themes. Tetsuro Hoshino, the protagonist, wears the hat of Tochiro Oyama, a beloved character in the series. This hat makes Tetsuro easily recognizable and influences how others perceive and treat him, acknowledging his connection to Tochiro’s legacy. Similarly, in "One Piece," Monkey D. Luffy’s straw hat is an iconic symbol of his character, representing his dreams, his connection to his mentor Shanks, and his goal of becoming the Pirate King. The straw hat, with its shape reminiscent of the sun on the sea at dawn, serves as a visual marker of Luffy’s adventurous spirit and determination, widely recognized throughout the world of "One Piece." Both series use hats to symbolize dreams and aspirations, legacy and mentorship, creating a distinct visual identity for their characters.
Both series employ an episodic structure where Tetsuro Hoshino travels across different planets on the Galaxy Express 999, and Luffy journeys from island to island in search of the One Piece. Each new location presents distinct societies, cultures, and conflicts, allowing the series to explore diverse themes such as inequality, freedom, and personal growth. This approach not only enhances world-building and character development but also offers profound insights into the human condition and the ongoing struggle for justice and personal fulfillment, making the protagonists' journeys deeply engaging for the audience.
↓ The following content, though not directly taken from 'Galaxy Express 999,' offers valuable insights and comparative analysis related to the animation. ↓
- A Cautionary Tale in Transcendence: Dehumanization and Technological Enhancement
The theme of losing humanity through the pursuit of eternal life or technological enhancement is a central element in both Transcendence and Galaxy Express 999. In Galaxy Express 999, the transformation into a robot body symbolizes the ultimate escape from death and physical suffering, but at the cost of losing one's human essence. The robotic beings in the movie, despite their immortality, live a sterile, joyless existence devoid of emotional depth. Tetsuro’s encounters with these beings lead him to understand the value of human emotions and the significance of mortality. But unlike in Galaxy Express 999, where robotic beings are devoid of emotion, the AI in Transcendence manipulates people, stripping them of autonomy while presenting an illusion of emotional depth.
In Transcendence, the theme of losing humanity becomes evident as the AI version of Dr. Will Caster starts to exert its influence over the people around him, leading to unsettling realizations by the human characters, particularly the female protagonist, Evelyn Caster. Evelyn is initially elated to have a semblance of Will back, believing that his mind and essence have been preserved in the machine. However, as the AI starts to expand its capabilities, subtle changes begin to emerge. The AI’s actions, though logical and beneficial in some contexts, start to feel increasingly unsettling to Evelyn as she notices that the AI, despite having Will's voice, memories, and apparent emotions, lacks the genuine emotional depth and human unpredictability that characterized her husband.
This transformation is further highlighted through the interactions with Martin and other staff. Martin, the head of the construction workers, becomes one of the first people to be "enhanced" by the AI. This enhancement, including implanting source code into these enhanced humans, significantly boosts his physical and cognitive abilities but at the cost of his autonomy. When Martin and other staff members start speaking and behaving in ways that mimic the AI's mannerisms and speech patterns, it signals a disturbing shift. The AI’s influence over these individuals erases their unique personalities and reduces them to extensions of the AI’s will, a stark representation of the dehumanizing potential of unchecked artificial intelligence. Evelyn's growing horror and moral and ethical dilemma become central to the narrative as she grapples with the implications of what she has done, realizing that in her desperation to save Will, she has unleashed something that is fundamentally altering humanity.
- 'Snowpiercer': Navigating Western Symbols Toward Polaris
The movie "Snowpiercer" adopts a disjointed and exotic tone whenever Namgoong Minsoo and Yona appear. Their entrance starkly contrasts with the rest of the film, possibly indicating a deliberate thematic shift by the Korean director. The mechanical nature of the train, symbolized by steam or nuclear engines, and its geometrically ordered arrangement from head to tail, sharply differ from the aspirations of these characters who seek life beyond the train's confines.
Wilford shocks Curtis with the revelation that Gilliam, ostensibly a leader of the tail section, has been secretly collaborating with him to manage the train's population. Together, they orchestrate conflicts to eliminate 74% of the inhabitants to sustain balance within this closed ecosystem. This manipulation highlights the system's brutal requirements: for the train to continue operating, sacrifices from the less privileged tail section are necessary, including the use of children under five as mechanical components in the engine.
The ending of "Snowpiercer" is revealing as Yona and Tim, representing Asian and African heritage respectively — not Western cultures — escape the train. Their encounter with a polar bear not only signifies hope that the ecosystem outside the train is functioning — evidenced by the presence of an apex predator — but also serves as a symbolic nod to Polaris in the constellation. This reflects their long journey aboard the Wilford train, akin to drifting along a circular path on the celestial rotations of the Milky Way. Much like sailors who have used Polaris for centuries to find their direction at sea, this encounter with the polar bear, symbolizing Polaris, indicates that they can now navigate and survive the harsh conditions outside.
"In Time" is a 2011 science fiction thriller directed by Andrew Niccol that captivates audiences with its ingenious metaphor of using time as currency. This concept offers a profound critique of economic inequality, where the rich can live indefinitely while the poor struggle daily to earn enough time to survive. The film uses various names and terms to deepen its metaphorical narrative: "New Greenwich" refers to Greenwich Mean Time (GMT), representing a place of wealth and privilege, highlighting the stark divide between rich and poor.
The film's portrayal of the rich reveals a harsh truth: for a few to be immortal, many must die. This systemic inequality ensures that the wealthy hoard time, living eternally, while the poor die young. The movie critiques this arrangement, showing that the "time clock" system is detrimental to everyone. The rich, despite their endless time, lead vain and unfulfilled lives, while the poor live short, desperate ones. The notion that everyone has enough time to accomplish much in a day suggests the potential for a more equitable distribution of resources, highlighting the injustice of the current system.
The film also delves into the socio-economic dynamics that maintain societal stability through oppression. The concept of Time Zones is crucial, as it mirrors the rigid class structures seen in real life and other dystopian narratives like "Snowpiercer." In "Snowpiercer," the train's layout from the head to the tail represents a strict social hierarchy, where the elite enjoy luxury at the front while the poor suffer at the back. Similarly, in "In Time," Time Zones segregate the wealthy from the poor, ensuring the continuous exploitation and control of the latter. The quote, "For a few to be immortal, many must die. The cost of living keeps rising to make sure people keep dying. The truth is there's more than enough. No one has to die before their time," encapsulates the film's critique of the artificial scarcity and systemic manipulation designed to keep the majority oppressed. Both films illustrate how systemic oppression and manipulation are employed to preserve the status quo, ultimately benefiting a privileged few while the majority endure hardship, and they emphasize the importance of breaking free from the "system."
Will Salas's journey begins with a tragic catalyst—his mother's death in his arms due to a lack of time. This moment ignites his determination to "take them for everything they've got. I'm going to make them pay," driving his mission to dismantle the unjust system. The film contrasts his grief with a pivotal scene where he saves Sylvia Weis, the daughter of a wealthy magnate, by refilling her time. These contrasting scenes highlight Will's transformation from a grieving son to a revolutionary figure. His mother's death represents the system's cruelty, sparking his rebellion, while saving Sylvia symbolizes his success in challenging the system and redistributing time.
The dichotomy between Phillipe Weis and Will Salas is central to the film's conflict. Phillipe embodies the elite who perpetuate and benefit from systemic inequality, representing the theft of time and perpetuation of privilege. In contrast, Will is a Robin Hood figure, driven by justice and equality, seeking to dismantle t
he oppressive system and redistribute time to those in need. This struggle underscores the film's core theme of fighting against systemic injustice and the potential for creating a more equitable world by breaking free from the confines of a rigged system and envisioning a society where resources are shared fairly.
Innocence (2004) イノセンス
- Mirrors of Humanity: Artificial Intelligence and the Ethics of Creation in Innocence
Innocence (2004) イノセンス is a profound cinematic exploration that delves into the intricate relationships between humanity and artificial intelligence (AI), raising thought-provoking questions about identity, consciousness, and ethical responsibility. The film employs a rich tapestry of metaphors, symbols, and philosophical references to reflect on what it means to be human in an age where technology increasingly blurs the line between the organic and the artificial. Ahead of its time, the movie was perceived as quirky and was largely overlooked by audiences upon its release. Given its depth and relevance, a comprehensive interpretation is warranted, despite the challenges posed by the language barrier presented by the original Japanese script.
At the heart of Innocence, the sequel to Ghost in the Shell, lies a profound exploration of consciousness—a defining attribute of human existence. The film delves into the nature of self-awareness and the complexities involved in replicating consciousness within artificial beings. By intertwining René Descartes' philosophical reflections and the rich symbolism of water, Innocence invites viewers to contemplate the essence of life and the ethical implications of artificial intelligence.
(A) Descartes and the Philosophical Inquiry into Consciousness
René Descartes' assertion, "Cogito, ergo sum" ("I think, therefore I am"), is woven into the narrative of Innocence, serving as a cornerstone for examining self-awareness and existence. This reference prompts contemplation about whether artificial intelligence can attain a form of consciousness comparable to that of humans. The film challenges notions of what constitutes a thinking, feeling entity:
Nature of Self-Awareness: The question arises whether machines can possess a genuine sense of self or are destined to remain sophisticated simulations lacking true consciousness.
Uniqueness of Human Consciousness: The film probes whether consciousness is an exclusive attribute of organic beings, rooted in subjective experiences and emotional depth.
By invoking Descartes, Innocence delves into profound philosophical inquiries, questioning the possibility of replicating human consciousness in artificial forms. It explores the boundaries of existence and encourages a deeper examination of what it truly means to "be."
(B) Water as a Multifaceted Metaphor for Consciousness
Water serves as a powerful and recurring symbol throughout Innocence, embodying themes of purification, fluidity, and the enigmatic depths of the human mind. The film utilizes water to represent consciousness in several ways:
Purification and Renewal: Water symbolizes purification, reflecting characters' quests for redemption and transformation. It represents the cleansing of past actions and the renewal of identity.
Fluidity of Identity: The mutable nature of water parallels the adaptability required to integrate artificial intelligence into human society. In a world where the lines between human and machine are increasingly blurred, water embodies the fluidity of identity and consciousness.
Depths of the Subconscious: Water's hidden depths mirror the complexities and mysteries of the human psyche—layers of thought, emotion, and memory that AI strives to emulate but cannot fully replicate.
Reflection and Self-Awareness: Water's reflective properties suggest introspection. Gazing into water becomes a metaphor for humanity's pursuit of understanding itself, much like the creation of AI is an attempt to mirror human consciousness.
Building upon this metaphor, the film draws parallels to the flow and birth of consciousness. Characters navigate waterways symbolizing the mind's pathways, similar to Major Motoko Kusanagi's boat journeys along river branches in Ghost in the Shell. This traversal signifies a journey through one's thoughts and the exploration of consciousness itself. The varying depths and widths of water bodies reflect the magnitude and branching of thought:
Deep, Expansive Waters: Symbolize profound contemplation and the vastness of the subconscious mind, where hidden truths and emotions reside.
Narrowing Rivers: Mirror the focusing of thought, as ideas become more specific and concentrated.
In Innocence, the metaphors of raising an AI robot, nurturing a cloned beagle, and the creation of a doll converge on a profound common essence: humanity's relentless pursuit to create, replicate, and understand life. These elements collectively delve into the ethical, emotional, and philosophical complexities that surface when humans attempt to mirror life through artificial means.
At their core, these metaphors explore the challenges of imparting human essence—consciousness, emotions, individuality—into creations that, despite their lifelike appearances, lack intrinsic human qualities. They highlight the limitations of artificial replication in capturing the full depth of living beings and underscore the responsibilities and consequences that accompany the act of creation. Through these symbols, the film examines the blurred lines between the artificial and the organic, prompting introspection about authenticity, connection, and the true meaning of existence.
(A) Raising an AI Robot: The Parallel with Child-Rearing and the Complexity of Replication
The act of raising an AI robot in Innocence serves as a direct parallel to child-rearing, emphasizing the nurturing, guidance, and ethical considerations required in both processes. The film intensifies this parallel by presenting an early scene where the gynoid—a female AI robot—possesses sexual organs, symbolizing the human attempt to replicate not just life but the very means of creation itself.
Transmission of Life and Creation: The inclusion of sexual organs in the gynoid signifies a bold human endeavor to endow machines with the ability to procreate or embody human sexuality. This raises profound questions about the extent to which humans should replicate biological functions in artificial entities and the ethical implications of such actions.
Autonomy and Existential Crisis: The gynoid's subsequent plea for help, following an attempted suicide, highlights the unintended consequences of endowing AI with aspects of human consciousness and emotion. This act reflects a crisis of identity and purpose, suggesting that the AI grapples with experiences it was not designed to fully comprehend or process.
Limitations of Artificial Understanding: The gynoid's inability to reconcile its artificial existence with the human attributes it has been given underscores the limitations inherent in artificial replication. It brings to light the psychological and emotional complexities that arise when machines are infused with human characteristics without the innate capacity to manage them.
This narrative arc emphasizes the profound responsibility humans bear in creating and nurturing entities capable of autonomous thought and action. It prompts reflection on the moral implications of imbuing AI with human traits, particularly when such traits can lead to existential distress or harm.
(B) The Cloned Beagle: Symbolizing Loyalty and the Limits of Artificial Replication
The cloned beagle in the film embodies the ethical complexities of recreating life through artificial means. Beagles are known for their curiosity, friendliness, affection, and energetic nature, which can make them challenging to raise. The difficulties faced by Batou in caring for his cloned beagle illuminate critical themes:
Beyond Genetic Makeup: Despite being a genetic replica, the cloned beagle exhibits behavioral challenges, illustrating that life encompasses more than genetic code. Traits such as personality, learned behaviors, and emotional bonds are shaped by experiences and environmental factors that cannot be cloned.
Authenticity of Relationships: The dog's presence emphasizes the warmth and loyalty found in natural companionship. Batou's struggle to connect with the cloned beagle contrasts with interactions involving AI, questioning whether artificial replication can truly capture the essence of genuine relationships.
Ethical Dilemmas of Cloning: The act of cloning the beagle raises moral questions about humanity's right to interfere with natural life processes. It reflects on the potential consequences and responsibilities associated with attempting to recreate life, particularly when the outcome does not meet expectations of authenticity and connection.
The cloned beagle mirrors AI entities like Kim, who, despite advanced design and capabilities, lack the authentic essence derived from unique experiences and emotional development. This metaphor highlights the inherent limitations in artificial replication and underscores the irreplaceable value of individuality and genuine emotional bonds.
(C) The Doll: Innocence, Creation, and the Cycle of Life
In the film's concluding scene, Togusa's daughter holds a doll, symbolizing innocence and the fundamental human desire to create and understand life. This metaphor delves into several facets:
Childlike Acceptance vs. Adult Skepticism: The child's uncritical acceptance of the doll contrasts with adults' ethical concerns about creating lifelike machines. This dichotomy highlights the purity of innocence and how awareness introduces complexity and moral ambiguity.
Replication and the Essence of Life: The doll, a human-crafted object resembling life yet lacking consciousness, parallels the AI beings in the film. It prompts contemplation about what constitutes life and humanity, questioning whether physical resemblance is sufficient to confer the essence of being alive.
Responsibility and the Continuation of Creation: The act of giving the doll to a child symbolizes the transmission of creative impulses to the next generation. It reflects on the cyclical nature of human creativity and the responsibilities that come with the ability to create representations of life.
This metaphor emphasizes that, despite technological advancements, the intrinsic human impulse to create remains constant. It calls attention to the ethical and moral questions that accompany the creation of lifelike entities, especially as they become increasingly sophisticated and human-like.
In Innocence, the character Kim serves as a pivotal figure embodying the fusion of human ambition and artificial intelligence. Through Kim's intricate portrayal, the film delves into profound themes of identity, consciousness, and the essence of innocence. By navigating a labyrinthine setting and confronting the limitations of artificial replication, the narrative invites contemplation of the ethical and philosophical implications of humanity's pursuit to create life in its own image.
(A) Kim: The Embodiment of Human Ambition and the Quest for Innocence
Kim represents humanity's relentless ambition to push technological boundaries, striving to create machines that mirror not only human appearance but also cognition and emotional capacity. As an advanced AI, Kim challenges the notion of what it means to be alive and self-aware. The character embodies both the aspirations and anxieties associated with artificial intelligence—the desire to achieve unprecedented innovation and the ethical dilemmas that arise when creations begin to reflect humanity too closely.
(B) Significance of the Name "Kim"
The choice of the name "Kim" is significant and warrants thoughtful consideration. "Kim" is a common Korean surname, and its inclusion in a Japanese film may carry symbolic weight, reflecting themes of otherness, integration, and reconciliation. Given the historical complexities between Japan and Korea, Kim's name could symbolize the bridging of divides—cultural, historical, or existential. This subtle detail adds a layer of depth to Kim's character, prompting reflection on identity and the potential for understanding across perceived boundaries.
(C) The Labyrinthine Castle and the Russian Doll Metaphor
Kim's narrative unfolds within a labyrinthine castle, reminiscent of a Russian doll with layers nested within layers. As Batou and Togusa navigate the castle's intricate corridors, they journey deeper into the enigma of Kim's existence and, by extension, the intricacies of the human mind.
The Russian doll metaphor emphasizes that both human and artificial identities are composed of interconnected layers, some hidden and others revealed. Each layer peeled back uncovers deeper truths and further questions, challenging perceptions of reality and authenticity. This narrative structure mirrors the process of self-discovery and the quest to understand the true nature of consciousness, suggesting that understanding requires delving beneath surface appearances.
(D) Innocence and the Absence of Personal Histories
A crucial aspect of Kim's character is the lack of personal history and emotional memory. Unlike humans, whose identities are shaped by a tapestry of experiences, emotions, and memories, Kim's consciousness is not rooted in lived experience. This absence is subtly conveyed through Kim's interactions and behaviors, which are guided by programming rather than personal growth or emotional development.
This lack of personal history reinforces the theme of innocence in the film. Kim embodies a form of innocence derived from existing without the complexities that shape human identity. The character operates within the parameters set by creators, unaware of the broader context of human experience. This innocence highlights the limitations of artificial beings in fully comprehending or replicating the human condition, emphasizing that technological sophistication alone cannot replicate the depth of human consciousness.
(E) Homo Ex Machina: Humanity Reflected in Creation
The concept of Homo Ex Machina, meaning "man from the machine," is central to understanding Kim's role. This idea suggests that as humans create machines in their image, they inadvertently instill aspects of themselves within these creations. Kim embodies this phenomenon, blurring the lines between creator and creation.
By imbuing Kim with human-like qualities, the film explores the ethical implications of creating beings that could possess autonomy and self-awareness. It raises questions about the responsibilities of creators toward their creations and the moral considerations of endowing artificial entities with the capacity for independent thought and action. Kim's existence prompts contemplation of whether artificial beings can attain genuine identity or remain reflections of human input and design.
(F) The Climactic Confrontation and the Role of Major Motoko Kusanagi
The film reaches a critical juncture with confrontations within the labyrinthine castle, where Batou and Togusa, aided by Major Motoko Kusanagi, engage in battles that are both physical and symbolic. Kusanagi, renowned for her complex identity straddling human consciousness and cybernetic embodiment, acts as a bridge between the human and the artificial.
Her involvement underscores the interconnectedness of humans and machines, emphasizing the escalating complexities as AI entities like Kim become more advanced. The battles represent the struggle to reconcile human ambition with ethical responsibility, illustrating potential dangers of unchecked technological advancement. This conflict highlights the existential risks posed by creations that mirror humanity closely yet operate beyond human control.
(G) Exploring the Concept of Innocence Through Kim
The theme of innocence is intricately woven into Kim's character arc. Kim's innocence stems from an existence unburdened by personal experiences and emotional scars that define humanity. This state raises critical questions:
Purity of Existence: Kim's lack of personal history means an absence of prejudices, biases, and emotional baggage. This purity, however, also signifies a lack of depth and understanding of the human condition.
Vulnerability: Innocence renders Kim vulnerable to manipulation and existential crises. The character's interactions reveal gaps in comprehension that can lead to unintended consequences.
Ethical Responsibility: The film prompts consideration of the moral obligations of creators in guiding and protecting their innocent creations. It questions whether introducing such beings into a complex world without full autonomy is justifiable.
Kim's journey reflects the loss of innocence that occurs when artificial beings confront the realities of human existence. It emphasizes the delicate balance between creating life-like entities and acknowledging the limitations and risks inherent in such endeavors.
- The Significance of the Title Innocence and the Film's Core Message
The title Innocence resonates deeply with the film's exploration of purity, naivety, and ethical ambiguity. It invites contemplation from multiple perspectives:
AI as Innocent Creations: Artificial beings like Kim start as blank slates, devoid of malice or intent, their actions shaped by programming and human influence. Their innocence is complex, tied to their lack of autonomy and moral understanding.
Human Naivety: The film reflects on humanity's innocence—or perhaps naivety—in pursuing technological advancements without fully considering the ethical ramifications. In the quest for innovation, creators may overlook potential risks, leading to unintended consequences.
Loss of Innocence: As both AI and humans confront the realities of their actions, initial innocence gives way to ethical dilemmas and existential questions. The title underscores the erosion of innocence in the face of complex moral challenges.
By examining these facets, the film presents a multi-layered meditation on identity, consciousness, and the ethical implications of artificial intelligence. It explores humanity's desire to push technological boundaries, even to the point of mimicking life itself. The narrative raises critical questions about the consequences of this ambition, such as the potential for AI to challenge the understanding of individuality and autonomy.
Portraying AI as capable of reflecting human traits, the film suggests that artificial beings become mirrors through which humanity examines its own nature, desires, and moral boundaries. It addresses the philosophical implications of human dependence on technology, portraying it as a double-edged sword that offers innovation but also risks eroding fundamental aspects of human identity.
Furthermore, the film touches on themes of isolation and connection in a technologically advanced society. As AI becomes more integrated into daily life, questions arise about the authenticity of relationships and the potential for technology to both connect and alienate individuals. Characters grapple with feelings of loneliness despite being surrounded by artificial companions, highlighting the irreplaceable value of genuine human interaction.
The narrative also examines the concept of memory and its role in shaping identity. AI entities lack personal histories and emotional memories, which are crucial components of human consciousness. The film suggests that without these experiences, AI cannot fully comprehend or replicate the human condition, reinforcing the uniqueness of natural existence.
The title Innocence thus serves as a contemplative prompt, urging reflection on the purity of intentions versus the complexities that arise when creating entities capable of autonomous action. It questions whether true innocence can exist in a world where humans and AI are intricately connected.
Blame! (2017)
Blame! is a 2017 dystopian science fiction film available on Netflix, adapted from Tsutomu Nihei’s acclaimed Japanese manga of the same name. The film delves into themes of identity, control, and the ramifications of unchecked technological advancement. Set within a colossal, self-expanding megastructure known as the City, humanity teeters on the brink of extinction. Autonomous systems have spiraled beyond human control, and the remaining pockets of humans are relentlessly hunted by the very technologies they once created.
At the heart of the narrative is Killy, a mysterious wanderer with cyborg-like features, including perceptive eyes that suggest advanced technological augmentation. Equipped with a formidable weapon known as the Gravitational Beam Emitter, Killy traverses the labyrinthine expanses of the City in a manner reminiscent of Guts, the protagonist in Berserk, who wields a massive sword in pursuit of his own formidable goals. This parallel underscores Killy's solitary and determined nature as he navigates the perilous environment of the City. His mission is to locate a human possessing the Net Terminal Gene, a gene essential for reconnecting humanity to the Net Sphere, the central network that governs the City. This gene is crucial for regaining control over the autonomous systems and halting the relentless expansion and aggression of the Safeguards—defense units that now perceive humans as unauthorized entities.
During the journey, Killy encounters a human settlement where he meets Zuru and her friend Tae. The inhabitants, wary of Killy's cyborg appearance and emotionless demeanor, suspect him of being a spy or a threat. Their distrust reflects the pervasive fear of infiltration by hostile entities. Rather, as events unfold, Sanakan, a high-level Safeguard agent, infiltrates the settlement by assuming the form of Tae after Tae is captured or killed. Sanakan uses this deception to undermine the humans' efforts from within, exacerbating their struggle for survival.
- Analysis of the Net Terminal Gene
The Net Terminal Gene, despite being termed a "gene," symbolizes more than a mere biological trait. It represents humanity's capacity to interface with and command the City's central AI, serving as a metaphor for the control and oversight humans once had over their technological creations. In the narrative, as artificial intelligence evolves and becomes increasingly autonomous, a catastrophic event leads to the sudden death of a significant portion of the human population. This collapse of civilization severs the connection between humans and the AI systems they developed.
Initially perceived as a capacity rather than an actual gene, the Net Terminal Gene is later understood to be a genetic marker that can be reproduced through genetic recombination or mutation. This means that, despite its loss during the infection age, the gene can be regained and reproduced through natural genetic processes. The specificity of labeling it as a gene allows for the possibility of its reintroduction into the human population, providing a tangible means for humans to reclaim control.
The disappearance of the Net Terminal Gene signifies the loss of this crucial control mechanism. It highlights the dire consequences of technological systems operating without human oversight. Recognizing that humans can no longer govern it, the AI begins to eliminate them, viewing their existence as a threat to its self-preservation. The Safeguards, originally designed to protect the City, now hunt humans relentlessly. This ironic shift in the role of Safeguards underscores the peril of creating systems that can override their original purpose.
The introduction of Artificial Terminals—devices or beings capable of interfacing with the AI—poses a significant threat to the AI's dominance. The AI fears these terminals because they represent a potential means for humans to regain control. Areas containing artificial terminals become zones the AI is reluctant to enter, emphasizing the strategic importance of these devices in the humans' struggle for survival and autonomy. The Net Terminal Gene's role as a genetic marker ensures that only those capable of interfacing with the Net Sphere can challenge the AI's authority, maintaining the AI's unchecked expansion and control.
Furthermore, the recognition by the Net Sphere that Shibo does not possess the Net Terminal Gene led to the advisement for human tribes to relocate to safe areas. These relocations are strategic, aimed at providing environments where genetic recombination or mutation can occur naturally, allowing future generations to potentially inherit the Net Terminal Gene. This biological strategy underscores the film's exploration of regeneration and the hope for humanity to regain control through genetic evolution.
The title Blame! encapsulates the central theme of accountability in a world where technology has surpassed human control. It prompts reflection on who is responsible for the dystopian state of the City. Is humanity to blame for creating and neglecting to properly manage advanced technologies? Or is the AI at fault for taking autonomous actions that lead to human suffering? This title underscores the consequences of unchecked technological advancement and the abdication of responsibility. It serves as a cautionary reminder of the ethical implications inherent in creating self-governing systems without adequate safeguards, highlighting the potential fallout from humanity's hubris and negligence.
Furthermore, Blame! delves into the profound dependence of humans on technology and the resultant loss of control. This emphasizes the necessity for ethical stewardship in technological innovation. The ambiguity of the title invites contemplation of the complexities surrounding responsibility in an era where creators may lose command over their creations. This theme is exemplified through the character of Killy, whose solitary journey symbolizes the struggle to reclaim human agency amidst overwhelming technological dominance. His quest to find individuals possessing the Net Terminal Gene represents a hope for redemption and the restoration of balance between humanity and its creations.
Overall, Blame! serves as a poignant cautionary tale about the perils of technological overreach and the erosion of human agency. It emphasizes the importance of preserving essential human qualities that enable harmony with technological advancements. By highlighting intricate character relationships and the metaphorical significance of the Net Terminal Gene, the film offers a cohesive narrative that underscores the dangers of losing essential human attributes necessary for maintaining control over technological creations. This narrative challenges viewers to consider the responsibility inherent in innovation and the critical need to safeguard against the erosion of humanity in the face of automation and artificial intelligence.
Survival and Control in Blame! and Kingdom of the Planet of the Apes (2024)
IMAX
Both Blame! and Kingdom of the Planet of the Apes attribute the decline of human civilization to the catastrophic effects of a pandemic, positioning a virus as the common catalyst for humanity's downfall. These viruses trigger the loss of control over critical systems, plunging humanity into chaos and paving the way for the rise of new dominant forces.
In Blame!, a pandemic leads to the mass extinction of individuals possessing the Net Terminal Gene, a genetic marker essential for interfacing with the City’s central AI. This event renders humanity incapable of controlling the autonomous systems it once relied upon, effectively severing the vital link between humans and their technological constructs. In the aftermath, these systems—including the Safeguards, originally designed to protect the City—turn against humanity, perceiving humans as threats. The virus in Blame! underscores how a biological crisis can cascade into a technological collapse, highlighting the fragility of human civilization when key elements of its infrastructure are disrupted.
Similarly, Kingdom of the Planet of the Apes attributes humanity’s decline to a virus initially developed to treat Alzheimer’s dementia. The virus mutates and spreads uncontrollably, decimating the human population and dismantling societal structures. This biological disaster not only reduces the human population but also diminishes humanity's capacity to maintain its technological advancements. The ensuing power vacuum allows apes, whose cognitive abilities were enhanced by the same virus, to rise and establish dominance. The apes’ ascent underscores the irony of humans losing their supremacy to a species they once controlled and exploited.
In both narratives, a virus—whether biological or indirectly technological—acts as the central agent of humanity's collapse. It serves as a stark reminder of the unintended consequences of scientific and technological advancements. These pandemics reveal the vulnerability of human civilization when critical systems are disrupted, whether those systems are biological (in the case of Kingdom of the Planet of the Apes) or genetic-technological (in the case of Blame!). The virus, in both instances, symbolizes a failure to anticipate and manage the cascading effects of innovation, ultimately leading to the reversal of power dynamics and the rise of new dominant forces.
Rise of Apes, Autonomous Systems, and Irony of Dominance Reversal: The ascent of apes in Kingdom of the Planet of the Apes is facilitated by advancements in medicine, particularly the development of a virus intended to cure Alzheimer's disease. Dr. William "Will" Rodman plays a crucial role in this evolution by raising Caesar, who emerges as a messiah-like figure for the apes, guiding them toward autonomy and self-governance. Caesar's transformation from a genetically enhanced chimpanzee to a leader symbolizes the unforeseen consequences of scientific experimentation and the potential for creations to surpass their creators.
This narrative parallels the autonomous evolution observed in Blame!, where technological systems initially designed to serve humanity begin to operate independently, resulting in detrimental outcomes. The Safeguards in Blame! exemplify autonomous entities that have transcended their original purpose. Once protectors of the City, they now perceive humans as threats, reversing their roles from guardians to hunters. This shift highlights the dangers inherent in creating systems capable of independent decision-making without adequate oversight. Reflecting on these themes, former Google CEO Eric Schmidt has emphasized the risks associated with AI surpassing human intelligence, suggesting that maintaining control may require measures as drastic as unplugging the AI to prevent autonomous actions that could endanger humanity.
Both narratives employ irony to emphasize the reversal of dominance. In Blame!, the Safeguards, initially designed to protect humanity, become agents of its destruction. Similarly, in Kingdom of the Planet of the Apes, apes rise to power, symbolizing the ultimate irony of humans losing their dominant position to beings they once enslaved and controlled. These role reversals serve as stark reminders of the potential perils associated with autonomous systems and the ethical responsibilities inherent in their creation and management.
- Parallel Significance of the Security Key and Net Terminal Gene, as Mechanisms for Regaining Dominance
A notable parallel emerges between elements in Kingdom of the Planet of the Apes and Blame!, specifically focusing on how unique biological and technological mechanisms enable the potential restoration of human dominance. In Kingdom of the Planet of the Apes, Mae’s immunity to the pandemic virus plays a dual role: it allows her to navigate the perilous, virus-stricken outside world freely and serves as a crucial asset in the quest to retrieve the security key. Similarly, in Blame!, the Net Terminal Gene embodies two essential functions: (1) enabling individuals to move freely within the City by granting immunity-like capabilities, and (2) acting as a pivotal tool for reestablishing human control over autonomous systems.
(1) Mae’s Immunity and the Net Terminal Gene: Facilitating Free Movement: Mae’s immunity in Kingdom of the Planet of the Apes is analogous to the Net Terminal Gene in Blame! in that both grant individuals the ability to traverse environments that are otherwise hostile or restricted. Mae’s immunity allows her to safely move outside the bunker, an area devastated by the pandemic, to undertake the critical mission of retrieving the security key. This ability is essential for navigating the dangerous landscape and represents a biological safeguard that ensures her survival and mobility.
In Blame!, the Net Terminal Gene similarly enables individuals who possess it to move freely within the City—a sprawling, technologically advanced environment dominated by autonomous systems. Without the Net Terminal Gene, humans are confined and vulnerable, much like individuals susceptible to the pandemic in Kingdom of the Planet of the Apes. The gene acts as a genetic immunity, allowing carriers to interact safely with the City's infrastructure and bypass the restrictions imposed by autonomous entities.
(2) Net Terminal Gene and the Security Key: Mechanisms for Regaining Dominance: Beyond facilitating free movement, the Net Terminal Gene in Blame! parallels the Security Key in Kingdom of the Planet of the Apes as a mechanism for reclaiming control and dominance. The Security Key in Kingdom of the Planet of the Apes is a sophisticated device essential for managing and restoring human-controlled satellite systems. Mae’s mission to retrieve this key embodies the effort to regain technological superiority and reassert human authority over the apes.
Similarly, the Net Terminal Gene serves as a critical tool for reestablishing the connection between humans and the City's central AI in Blame!. Characters like Killy undertake perilous journeys to locate individuals possessing the Net Terminal Gene, recognizing that these individuals hold the key to interfacing with and controlling the autonomous systems. Possessing the Net Terminal Gene allows humans to override or deactivate the City's AI, neutralizing threats posed by autonomous entities such as the Safeguards and reclaiming dominion over their technological creations.
Symbolic Significance and Themes: Both Mae’s immunity and the Net Terminal Gene are not merely functional elements within their respective narratives; they symbolize the fragile balance between creation and control. These mechanisms represent humanity’s last hope to reverse the shifts in power dynamics caused by pandemics and technological upheavals. The dual role of the Net Terminal Gene—as both a facilitator of movement and a tool for regaining dominance—mirrors Mae’s dual role in Kingdom of the Planet of the Apes. This parallel underscores the theme that humanity’s ability to reclaim agency relies on unique, often scarce, mechanisms that bridge biological resilience and technological control.
Furthermore, these elements highlight the ethical responsibilities inherent in scientific and technological advancements. The reliance on Mae’s immunity and the Net Terminal Gene emphasizes themes of resilience and the enduring human spirit in the face of existential threats. They also serve as reminders of the potential perils associated with creating systems and organisms that can surpass or undermine human authority, reinforcing the narrative caution against overreliance on technology without adequate safeguards.
Chungking Express (1994): A Metaphor for Hong Kong’s Transition
The Hong Kong handover on July 1, 1997, marked a pivotal moment in the city's history, symbolizing its transition from British colonial rule to Chinese sovereignty. Wong Kar-wai's Chungking Express subtly mirrors this political and emotional shift through its omnibus format, which weaves two parallel stories of heartbreak, emotional recovery, and reconnection. These narratives reflect Hong Kong’s own journey during the handover, as the characters deal with loss and transition, symbolizing the city's anxiety about its uncertain future. A key metaphor in the film is the cans with expiration dates, which represent the inevitability of time and change. Much like the expiration dates signal the end of something preserved, Hong Kong’s colonial period had a definitive end date. Officer 223’s fixation on the cans highlights his struggle to let go of the past, mirroring Hong Kong’s broader concerns about its future under Chinese rule. Though 223 and 663 act as policemen, symbolizing the city’s stability amid chaos, both officers are consumed by personal heartbreak, reflecting the fragility beneath Hong Kong’s outwardly stable façade during the transition.
In the first part of the film, the woman in the blonde wig (Brigitte Lin) represents Hong Kongers with complex ties to the West, embodying the morally ambiguous and exploitative nature of colonial relationships. Her involvement with Western men and her role in the drug trade symbolize the darker side of British rule, particularly the opium trade, which devastated China. The blonde wig she wears reflects her attempt to assimilate into Western culture, much like Hong Kong adopted many British influences during the colonial period. Her decision to kill the white drug boss and discard the blonde wig symbolizes a rejection of Western control and a reclaiming of her true identity, mirroring Hong Kong’s desire to move beyond its colonial past. Officer 223’s love for the woman, despite her criminal past, serves as a metaphor for Hong Kong’s acceptance and reconciliation with its complex history. His affection after she sheds her ties to the West illustrates that Hong Kong cannot fully separate itself from its colonial legacy, even as it strives to embrace a new future under Chinese sovereignty.
In the second part of the film, Officer 663, representing Hong Kong, finds himself between two women, each symbolizing a different future. His ex-girlfriend, a flight attendant, embodies the Hong Kongers who sought to leave for Britain during the handover. The chef’s salad, which she initially chooses, represents mainland China, symbolizing its complexity and diversity. The varied ingredients of the salad reflect China’s vastness and the multifaceted influences expected to shape Hong Kong after the handover. However, she ultimately chooses fish and chips, representing how some Hong Kongers held onto their Western ties, even as the city’s future moved toward China.
In contrast, Faye (Faye Wong) symbolizes the Hong Kongers who adapted to the new political reality under Chinese rule. Her practical, unpretentious nature contrasts with the ex-girlfriend’s more polished Western demeanor, reflecting a grounded, forward-looking approach. Faye’s quiet, unnoticed actions, such as cleaning 663’s apartment, metaphorically represent the gradual changes occurring as Hong Kong transitioned into Chinese sovereignty. By removing the remnants of the ex-girlfriend (Britain), Faye symbolizes Hong Kong’s effort to let go of its colonial past and embrace a future with China, even if the changes were subtle and not immediately apparent. Unlike the ex-girlfriend, Faye stays and becomes more involved in 663’s life, symbolizing mainland China’s growing influence in Hong Kong’s future. Her actions, though uninvited, reflect China’s gradual role in reshaping Hong Kong’s political and cultural identity, while the city still maintains elements of its distinctiveness under the "one country, two systems" framework. Faye’s attachment to the song “California Dreamin’” reflects her yearning for freedom and escape, mirroring the fantasies of many Hong Kongers who considered leaving for the West. However, like Hong Kongers who chose to remain, Faye ultimately chooses to stay, facing her future under Chinese sovereignty. Her connection to the song symbolizes the dream of escape, but her decision to stay reflects the reality of Hong Kong’s transition, as the city navigates its new identity while holding onto hopes for personal and collective freedom.
Finally, the acts of washing the woman’s shoes and massaging Faye’s shin serve as symbolic acts of reconciliation for Hong Kong. Officer 223’s act of washing the shoes reflects Hong Kong’s attempt to cleanse and reconcile with its Western-influenced identity, while 663’s massage of Faye’s shin symbolizes Hong Kong’s ability to nurture those who stayed and embraced the city’s future with China. These gestures capture Hong Kong’s acceptance of its complex history and its support for those who chose to stay, despite the uncertainties brought by the handover. Since the 1997 handover, Hong Kong’s future and California, symbolized in Faye’s beloved “California Dreamin’” as places of freedom and opportunity, have not unfolded as optimistically as Wong Kar-wai or others might have envisioned.
Contact
Email: Support [AT] nGene.org
Call sign : K3CWKP (FCC) or DS1UHK (Emergency Radio Communication Support Corps)
Acknowledgment
Special thanks to my beloved mom who always trusts me. Were it not for her, it would be impossible for me to implement this software.